
The Association Between Depression, Anxiety and COVID-19 Symptoms
Marilyn M. Bartholmae1,2*, Joshua, M. Sill3, Matvey V. Karpov1, Sunita Dodani1,4
1EVMS-Sentara Healthcare Analytics and Delivery Science Institute, Norfolk, VA, USA
2Department of Psychiatry and Behavioral Sciences, Eastern Virginia Medical School, Norfolk, VA, USA
3Division of Pulmonology, Department of Internal Medicine, Eastern Virginia Medical School, Norfolk, VA, USA
4Division of Cardiology, Department of Internal Medicine, Eastern Virginia Medical School, Norfolk, VA, USA
Abstract
Background: The variation of COVID-19 illness is not fully understood. There is a need for further identification of predictors for COVID-19-related health outcomes, which may improve the delivery of healthcare. The primary objective was to identify whether anxiety/depression symptoms are associated with the number of COVID-19 symptoms. The second objective was to examine differences in anxiety and depression symptoms between individuals with or without COVID-19 symptoms.
Methods: 782 Virginians ages 18 to 87 years, enrolled from March to May 2021 and were followed-up for six months. Vibrent Health online platform was used to collect data. PHQ-9, GAD-7, and CDC's COVID-19 tracing form, were used to assess depression, anxiety, and COVID-19 symptoms, respectively. An MMRM test was used to examine whether anxiety and depression symptoms were associated with the number of COVID-19 symptoms. Age, race, sex, medical diagnoses, and COVID-19 related economic/social hardships were included as covariates. Mann-Whitney U tests were used to assess differences in anxiety/depression at all study time points. We conducted analyses using SAS 9.4, p-values < .05 were considered significant.
Results: Depression/anxiety symptoms, COVID-19 related economic/social hardships, and medical diagnoses, were significantly associated with the number of COVID-19 symptoms (p<.05), whereas age, sex, and race were not (p>.05). Overall, PHQ9 and GAD7 scores were consistently and significantly higher for individuals with COVID-19 symptoms than those without COVID-19 symptoms (p<.05).
Conclusions: The severity of depression and anxiety symptoms is linked to symptoms of COVID-19 over time. Physical and mental health integrated healthcare approaches may be necessary. Further investigation into causative mechanisms is needed.
Introduction
Individuals with COVID-19 who have medical comorbidities1-5, older age1,4,5, or are from low socioeconomic status1-4, are at increased risk of experiencing COVID-19 related adverse health effects. Poverty is a risk factor for developing hypertension, cardiovascular disease, obesity, and hypertension1,2. These medical conditions are also risk factors for contracting COVID-191,2,4,6,7. Although there are predictors for COVID-19- related health outcomes, accurate prognostication is not possible8. The presentation of symptoms for acute COVID-19 or subsequent Long COVID varies from person to person9, regardless of hospitalization status10-12, SARS-CoV-2 variant type11, or COVID-19 vaccination status13.
Although some common symptoms for individuals with COVID-19 include fever, reduced general condition, dyspnea, and cough, COVID-19 shows significant variation. Individuals with COVID-19 could be asymptomatic, experience mild cold symptoms, develop Long COVID (defined as signs and symptoms for COVID-19, which persist more than four weeks from the onset of infection and result in an emerging health condition14), or have acute respiratory distress syndrome and death8,15. For example, among hospitalized patients, one study reported 14% of patients had atypical chest pain and 25% had symptoms of brain fog. Tissue abnormalities were noted in the lungs (60%), kidneys (29%), heart (26%), and liver (10%). Interestingly, younger age did not protect against Long-COVID9.
There is a need for identification of other confounding predictors for COVID-19- related health outcomes to improve the coordination of necessary delivery of healthcare services. There is growing evidence that poor psychological health may be linked to biological processes and behaviors, which cause and exacerbate disease16. Previous findings suggest mental health and physical health are interconnected16-19 by neural systems that jointly regulate somatic physiology and complex mental abilities18. People with mental illness are at higher risk for developing physical illness. For example, people with psychosis are more likely to smoke, have poor oral health, have cardiovascular risk factors, and increased risks of osteoporosis and sexual dysfunction. The increase in life expectancy in developed countries has not benefited people with psychosis, they are more likely to die 18 years earlier compared to the general population17. Conversely, individuals with chronic medical conditions such as diabetes, cardiovascular disease, and cancer, are at risk of developing mental illness. For example, individuals with diabetes are more likely to experience depression, anxiety, eating disorders, and cognitive impairments. When diabetes and eating disorder are comorbid, the mortality rate is seven times higher than the general population, and three times higher than individuals who have either diabetes or eating disorder alone17.
We hypothesized the severity of anxiety and depression symptoms may be associated with COVID-19 symptoms. We also hypothesized that social and economic hardships related to the COVID-19 pandemic, age, race, sex, and having diagnosed medical conditions, could confound how COVID-19 illness is experienced. This longitudinal study aims to 1) identify whether anxiety and depression symptoms are associated with the number of COVID-19 symptoms experienced in a longitudinal model, and 2) examine differences in anxiety and depression symptoms between individuals with or without COVID-19 symptoms at baseline and follow-ups one through six. Findings may inform the best healthcare delivery practices for COVID-19 patients with anxiety and/or depression. Integrated healthcare approaches such as disease management programs, coordination between services, integrated care team, and integrated care management, have been proposed as means to reduce healthcare costs and improve health outcomes for multimorbidity20. An integrated healthcare approach addressing COVID-19 with comorbid mental illness may result in improved clinical effectiveness and may reduce the burden of COVID-19 short- and long-term healthcare costs.
Methods
COVIDsmart Study
The statewide COVIDsmart Study is a digital study designed to evaluate the economic, social, clinical, and behavioral impacts of COVID-19 on Virginians and their communities. This study is a partnership between the Eastern Virginia Medical School (EVMS) - Sentara Healthcare Analytics and Delivery Science Institute (HADSI), George Mason University (GMU), and Vibrent Health Inc21.
Recruitment Strategies
A detailed methodology of COVIDsmart has been published previously21. Briefly, participants were recruited via online articles, employer e-newsletters, purchased email lists targeting racial/ethnic minorities, social media (e.g., Facebook, Instagram, and LinkedIn), television, and paper/digital flyers shared with multiple hospitals, churches, and other community organizations21.
Data Collection
The COVIDsmart study used an online data collection platform designed by Vibrent Health Inc. This platform was compliant with the Health Insurance Portability and Accountability Act. It required an Internet connection but no other software was required22. A total of 782 residents of Virginia, ages 18 to 87 years, enrolled from March to May 2021 with six months follow-up of study participants. The COVIDsmart study collected clinical, social, economic, and behavioral data. This study included participants who completed demographic information and the mood modules containing the Patient Health Questionnaire-9 (PHQ9) and the Generalized Anxiety Disorder-7 (GAD7). The PHQ923 and GAD724 are valid and reliable instruments to measure symptoms of depression and anxiety, respectively. Demographic and medical history data were collected at baseline. PHQ9 and GAD7 scores, COVID-19 symptoms, and social/economic hardship variables were collected at baseline and monthly follow-ups one through six.
The survey question for COVID-19 symptoms was adapted from the 2020 Center for Disease Control and Prevention (CDC)’s COVID-19 contact tracing form25. Symptoms listed included abdominal pain, chest pain, chills, cough (worse than usual), diarrhea, fatigue/general malaise, feeling feverish (not measured), fever (measured with a temperature ≥ 100.0 degrees F), headache, loss of appetite, loss of taste or smell, muscle/ joint aches or pains (worse than usual), nausea or vomiting, runny nose or extra mucus from the nose, scratchy or sore throat, shortness of breath or difficulty breathing/wheezing, or other symptoms.
Social and economic hardships were COVID-19 related negative experiences such as losing a job, inability to buy groceries, inability to visit family members at higher risk for infection, and other undesirable experiences caused by the pandemic. The survey questions to obtain the COVID-19 related economic and social hardships were created by an expert panel from GMU and EVMS, including an epidemiologist, a sociologist, a psychologist, a health services researcher, a cardiologist, and a pulmonologist. Survey questions were published by Bartholmae et al. 202221.
Research Ethics Approval
This COVIDsmart study received an expedited review and was approved by Eastern Virginia Medical School’s Institutional Review Board (IRB), an independent regulatory body established to protect human research subjects (IRB# 20-07-EX-0138-OTHER).
Statistical Analysis
Descriptive statistics were used to analyze the demographics of COVIDsmart participants. To examine the relationship between anxiety symptom severity, depression symptom severity, and the number of COVID-19 symptoms, a Mixed Methods Repeated Measures (MMRM) test was used. MMRM is a robust statistical procedure widely known in the literature as the most efficient statistical analysis to address the bias from missing data26-30. In this model, the dependent variable was the number of symptoms reported, the independent variables were PHQ9 and GAD7 scores, and the covariate variables were age, race, sex, number of medical diagnoses, and the number of COVID-19 related social and economic hardships. These covariate variables were selected as low socioeconomic status1-4, older age1,4,5, being a racial/ethnic minority1-4, being a male5, and having medical comorbidities1-5, are risk factors for COVID-19. The MMRM test was followed by a series of Mann-Whitney U tests to examine whether PHQ-9 and GAD-7 scores differed significantly between participants who reported one or more COVID-19 symptoms compared to participants who did not report any COVID-19 symptoms at baseline and follow-ups one through six. The number of social and economic hardships were included in the Mann Whitney U tests as they were a significant longitudinal covariate based on MMRM analysis. We conducted the analysis using SAS 9.4, and p values < .05 were considered significant.
Results
At baseline, the majority of participants were non-Hispanic White (89.3%) and female (78.14%). Mean values with respective standard deviations were as follows: age - 50 years (SD = 14.52), PHQ9 - 6.04 (SD = 5.67), GAD7 - 4.82 (SD = 5.08), and COVID-19 related hardships - 2.71 (SD = 1.81). The percent of participants remaining in the study from baseline were 66.37%, 53.66%, 44.54%, 37.22%, 35.28%, and 31.69% for follow-ups 1 through 6, respectively. Demographics for follow-ups 1 through 6 are in Tables 1 and 2.
Table 1: Descriptive Statistics for Categorical Variables for Each Study Time Point
|
Time Point |
Categorical Variables |
n (%) |
|
Baseline |
Sex |
|
|
|
Female |
522 (78.14%) |
|
|
Male |
146 (21.86%) |
|
|
Race |
|
|
|
White |
593 (89.31%) |
|
|
Black |
44 (6.63%) |
|
|
Other |
23 (3.45%) |
|
|
Prefer not to say |
4 (0.60%) |
|
Follow-Up 1 |
Sex |
|
|
|
Female |
351 (79.23%) |
|
|
Male |
92 (20.77%) |
|
|
Race |
|
|
|
White |
398 (90.25%) |
|
|
Black |
23 (5.22%) |
|
|
Other |
17 (3.86%) |
|
|
Prefer not to say |
3 (0.68%) |
|
Follow-Up 2 |
Sex |
|
|
|
Female |
281 (78.27%) |
|
|
Male |
78 (21.73%) |
|
|
Race |
|
|
|
White |
318 (89.33%) |
|
|
Black |
20 (5.62%) |
|
|
Other |
15 (4.21%) |
|
|
Prefer not to say |
3 (0.84%) |
|
Follow-Up 3 |
Sex |
|
|
|
Female |
235 (78.86%) |
|
|
Male |
63 (21.14%) |
|
|
Race |
|
|
|
White |
265 (89.83%) |
|
|
Black |
16 (5.42%) |
|
|
Other |
11 (3.73%) |
|
|
Prefer not to say |
3 (1.02%) |
|
Follow-Up 4 |
Sex |
|
|
|
Female |
194 (77.91%) |
|
|
Male |
55 (22.09%) |
|
|
Race |
|
|
|
White |
224 (91.06%) |
|
|
Black |
13 (5.28%) |
|
|
Other |
7 (2.85%) |
|
|
Prefer not to say |
2 (0.81%) |
|
Follow-Up 5 |
Sex |
|
|
|
Female |
183 (77.54%) |
|
|
Male |
53 (22.46%) |
|
|
Race |
|
|
|
White |
210 (90.13%) |
|
|
Black |
13 (5.58%) |
|
|
Other |
8 (3.44%) |
|
|
Prefer not to say |
2 (0.86%) |
|
Follow-Up 6 |
Sex |
|
|
|
Female |
164 (77.36%) |
|
|
Male |
48 (22.64%) |
|
|
Race |
|
|
|
White |
190 (90.91%) |
|
|
Black |
10 (4.78%) |
|
|
Other |
7 (3.36%) |
|
|
Prefer not to say |
2 (0.96%) |
Table 2: Descriptive Statistics for Continuous Variables for Each Study Time Point
|
Time Point |
Continuous Variables |
N |
Min |
Max |
µ ± SD |
Skewness |
Kurtosis |
|
Baseline |
Age |
667 |
18 |
87 |
50.61 (14.52) |
0.008 |
-0.821 |
|
|
PHQ9 |
669 |
0 |
26 |
6.04 (5.67) |
1.184 |
0.882 |
|
|
GAD7 |
664 |
0 |
21 |
4.82 (5.08) |
1.242 |
0.913 |
|
|
COVID-related hardships |
670 |
0 |
11 |
2.71 (1.81) |
1.037 |
1.145 |
|
Follow-Up 1 |
Age |
442 |
20 |
87 |
50.82 (14.99) |
0.047 |
-0.845 |
|
|
PHQ9 |
445 |
0 |
23 |
4.85 (5.06) |
1.421 |
2.01 |
|
|
GAD7 |
444 |
0 |
21 |
4.23 (4.64) |
1.377 |
1.412 |
|
|
COVID-related hardships |
445 |
0 |
8 |
1.35 (1.00) |
3.013 |
13.006 |
|
Follow-Up 2 |
Age |
358 |
20 |
87 |
51.89 (15.33) |
-0.039 |
-0.903 |
|
|
PHQ9 |
359 |
0 |
24 |
4.48 (4.91) |
1.565 |
2.661 |
|
|
GAD7 |
355 |
0 |
21 |
3.85 (4.47) |
1.592 |
2.639 |
|
|
COVID-related hardships |
360 |
0 |
7 |
1.18 (0.75) |
3.240 |
16.156 |
|
Follow-Up 3 |
Age |
297 |
20 |
87 |
53.22 (15.03) |
-0.194 |
-0.936 |
|
|
PHQ9 |
298 |
0 |
26 |
4.24 (4.91) |
1.694 |
3.462 |
|
|
GAD7 |
296 |
0 |
21 |
3.68 (4.54) |
1.790 |
3.299 |
|
|
COVID-related hardships |
298 |
0 |
6 |
1.11 (0.50) |
4.842 |
35.142 |
|
Follow-Up 4 |
Age |
248 |
20 |
83 |
54.83 (14.75) |
-0.325 |
-0.837 |
|
|
PHQ9 |
249 |
0 |
27 |
4.41 (5.16) |
1.810 |
3.808 |
|
|
GAD7 |
247 |
0 |
21 |
3.71 (4.46) |
1.611 |
2.662 |
|
|
COVID-related hardships |
249 |
0 |
5 |
1.14 (0.62) |
3.351 |
13.941 |
|
Follow-Up 5 |
Age |
235 |
22 |
83 |
55.46 (14.69) |
-0.331 |
-0.834 |
|
|
PHQ9 |
236 |
0 |
26 |
4.22 (4.87) |
1.800 |
3.949 |
|
|
GAD7 |
236 |
0 |
21 |
3.71 (4.42) |
1.720 |
3.154 |
|
|
COVID-related hardships |
236 |
0 |
4 |
1.05 (0.50) |
2.171 |
10.389 |
|
Follow-Up 6 |
Age |
212 |
22 |
83 |
64.89 (12.16) |
-0.362 |
-0.864 |
|
|
PHQ9 |
212 |
0 |
27 |
4.27 (5.11) |
1.886 |
4.345 |
|
|
GAD7 |
209 |
0 |
21 |
3.96 (5.06) |
1.741 |
2.702 |
|
|
COVID-related hardships |
212 |
0 |
4 |
1.13 (0.51) |
3.588 |
15.656 |
aAt baseline, three participants reported having previously diagnosed anxiety and depression.
Longitudinal data collected on the study participants over the course of six months demonstrated that the number of COVID-19 symptoms was associated with increased levels of depression symptoms (F=22.70, p<.0001), anxiety symptoms (F= 4.04, p = 0.045), and COVID-19 related economic/social hardships (F= 26.21, p<.0001). Having a diagnosed medical condition significantly confounded this result (F= 19.47, p<.0001). Age (F=0.19, p = 0.663), sex (F=0.29, p = 0.590), and race (F=0.94, p=0.490) were not associated with the number of COVID-19 symptoms experienced.
Figures 1 through 7 display differences in PHQ-9, GAD-7, and COVID-19-related social and economic hardships among participants with COVID-19 symptoms versus participants without COVID-19 symptoms. At every time point (baseline and follow-ups 1 through 6), PHQ9 scores were consistently and significantly higher for participants experiencing COVID-19 symptoms compared to participants without COVID-19 symptoms (p<.05). When breaking down the PHQ-9 by question, scores remained higher for participants with COVID-19 symptoms compared to participants without COVID-19 symptoms across all PHQ-9 questions and across all study time points (Table 3). GAD7 scores were consistently higher for participants with COVID-19 symptoms than for participants without COVID-19 symptoms (Table 4). Differences in GAD7 between the two groups were significant at baseline, follow-ups one through four, and follow-up six (p<.05) but not for follow-up five (p>.05). Except for follow-up three, the COVID-19 related economic/social hardships were higher for participants with COVID-19 symptoms. However, statistical significance between the two groups was only achieved at baseline and follow up one (p<.05). Overall, the severity of PHQ-9 and GAD-7 was higher for participants with COVID-19 symptoms compared to participants without COVID-19 symptoms.
Table 3: PHQ-9 Severity Groups Comparison between Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms
|
|
PHQ-9 (With COVID-19 Symptoms) |
PHQ-9 (No COVID-19 Symptoms) |
||||
|
|
Severe |
Moderately Severe |
Moderate |
Severe |
Moderately Severe |
Moderate |
|
Baseline |
8.72% (13/149) |
14.76% (22/149) |
16.78% (25/149) |
2.30% (12/521) |
4.80% (25/521) |
8.45% (44/521) |
|
FU1 |
6.82% (6/88) |
10.23% (9/88) |
17.05% (15/88) |
1.40% (5/357) |
2.24% (8/357) |
7.5% (27/357) |
|
FU2 |
5.88% (3/5) |
9.80% (5/5) |
5.88% (3/5) |
0.65% (2/310) |
2.26% (7/310) |
8.71% (27/310) |
|
FU3 |
2.63% (1/38) |
7.89% (3/38) |
21.05% (8/38) |
1.5% (4/260) |
1.5% (4/260) |
7.69% (20/260) |
|
FU4 |
2.70% (1/37) |
2.70% (1/37) |
10.81% (4/37) |
2.35% (5/212) |
3.30% (7/212) |
5.66% (12/212) |
|
FU5 |
3.7% (1/27%) |
0% (0/0) |
18.52% (5/27) |
2.87% (6/209) |
0.96% (2/209) |
6.22% (13/209) |
|
FU6 |
5.88% (2/34) |
0% (0/0) |
8.82% (3/34) |
1.69% (3/178) |
2.25% (4/178) |
8.43% (15/178) |
Table 4: GAD-7 Severity Groups: Comparison between Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms
|
|
GAD-7 (With COVID-19 Symptoms) |
GAD-7 (No COVID-19 Symptoms) |
||
|
|
Severe |
Moderate |
Severe |
Moderate |
|
Baseline |
19.46% (29/149) |
14.09% (21/149) |
3.45% (18/521) |
8.83% (46/521) |
|
FU1 |
7.95% (7/88) |
20.45% (18/88) |
3.98% (13/327) |
6.44% (23/357) |
|
FU2 |
7.84 % (4/51) |
11.76% (6/51) |
2.58% (8/310) |
6.77% (21/310) |
|
FU3 |
13.16% (5/38) |
7.89% (3/38) |
2.69% (7/260) |
5.77% (15/260) |
|
FU4 |
5.40% (2/37) |
16.21% (6/37) |
2.36% (5/212) |
6.60% (14/212) |
|
FU5 |
7.40% (2/27) |
3.70% (1/27) |
2.87% (6/209) |
6.70% (14/209) |
|
FU6 |
8.82% (3/34) |
8.82% (3/34%) |
5.62% (10/178) |
5.62% (10/178) |
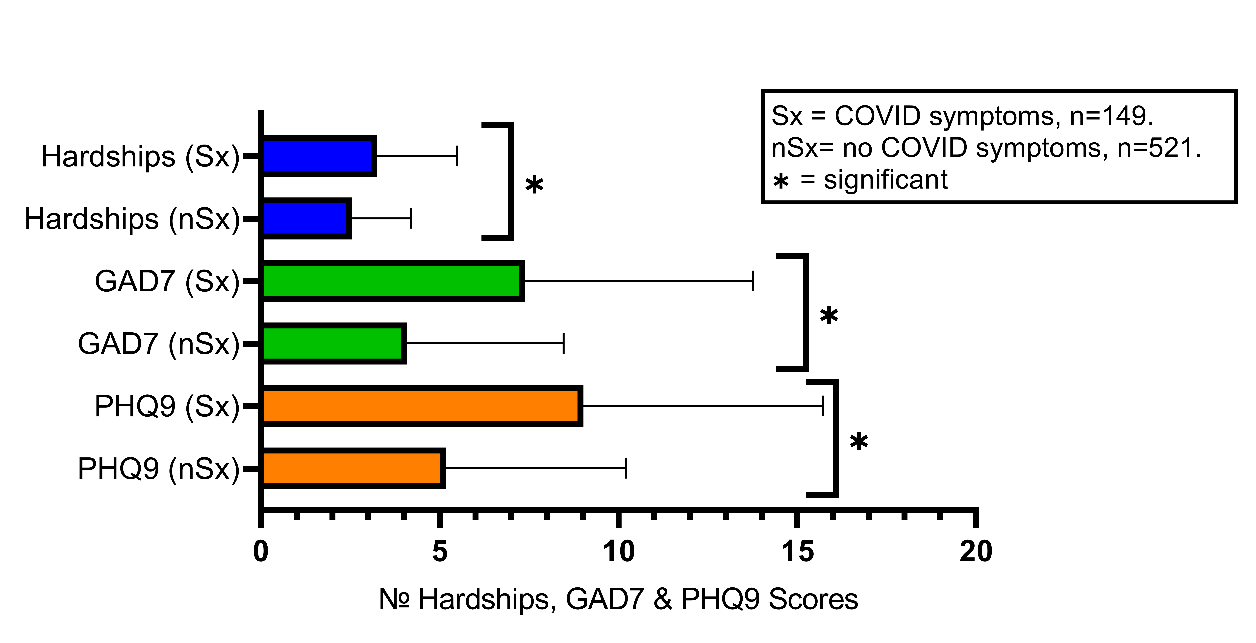
Figure 1: Baseline: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
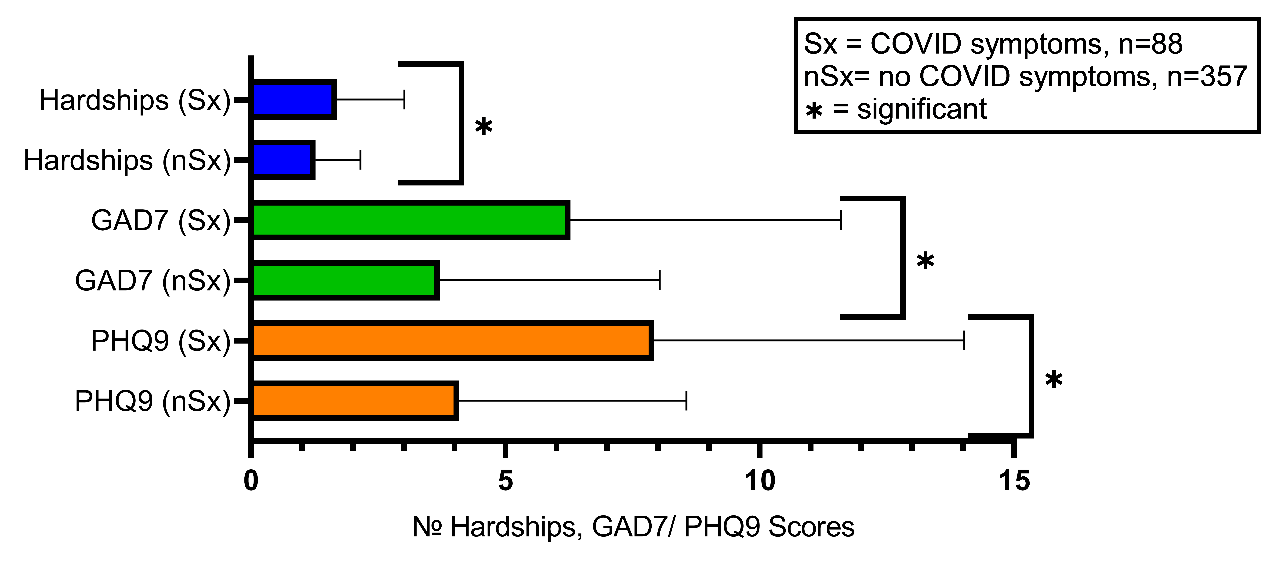
Figure 2: Follow-up #1: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
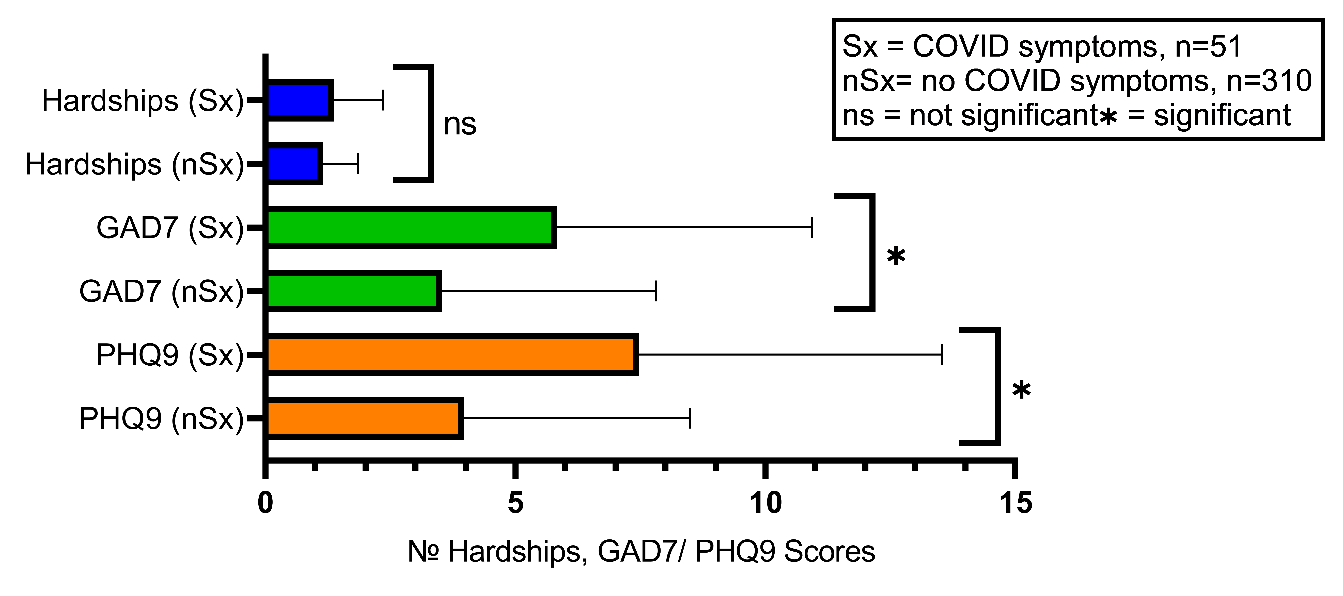
Figure 3: Follow-up #2: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
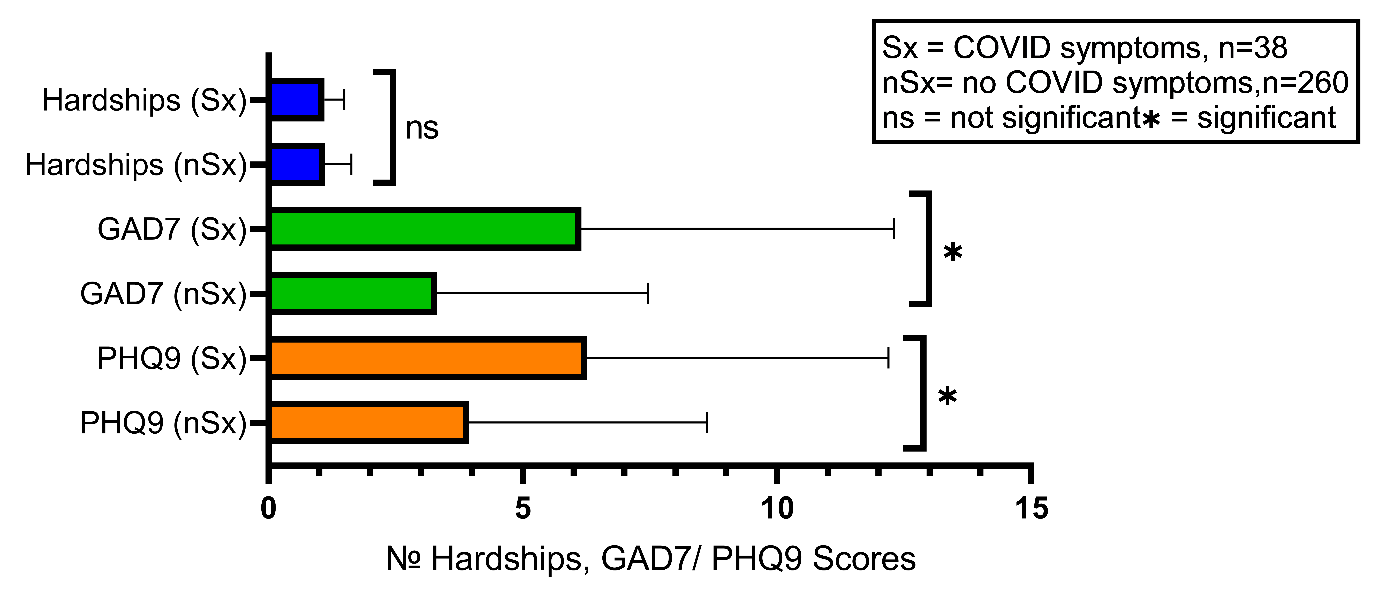
Figure 4: Follow-up #3: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
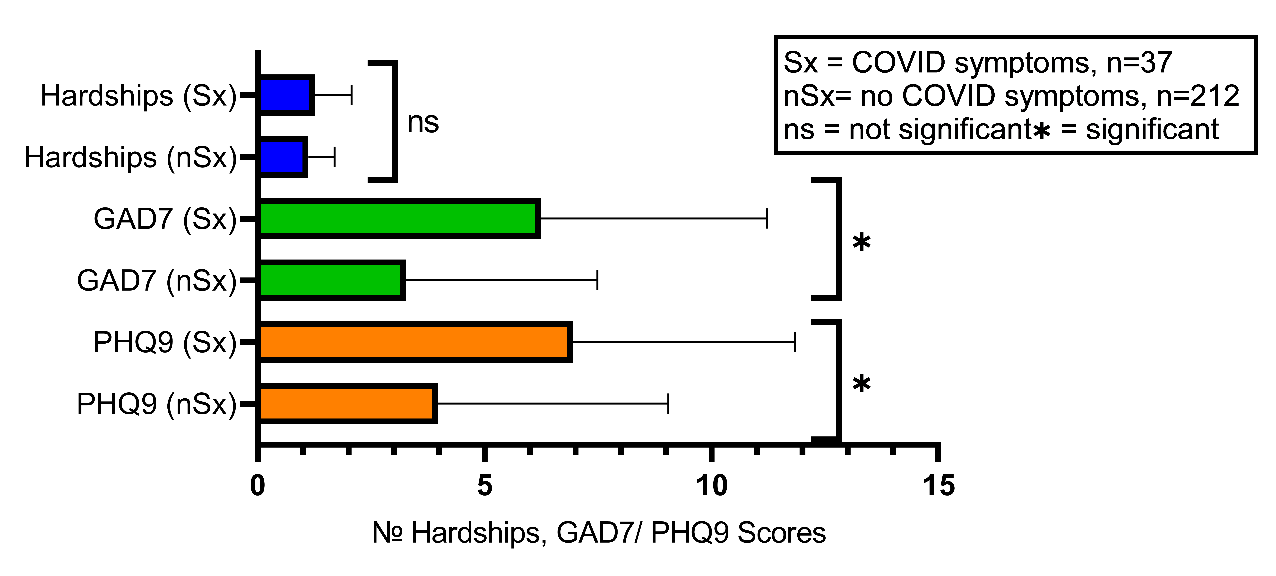
Figure 5: Follow-up #4: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
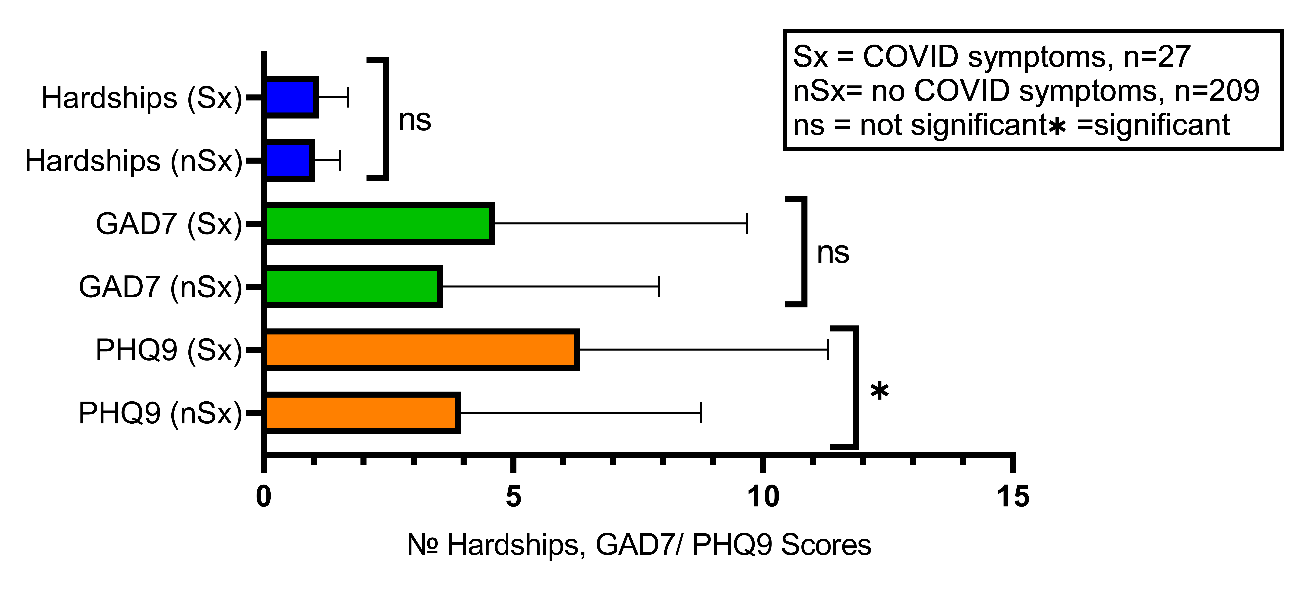
Figure 6: Follow-up #5: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
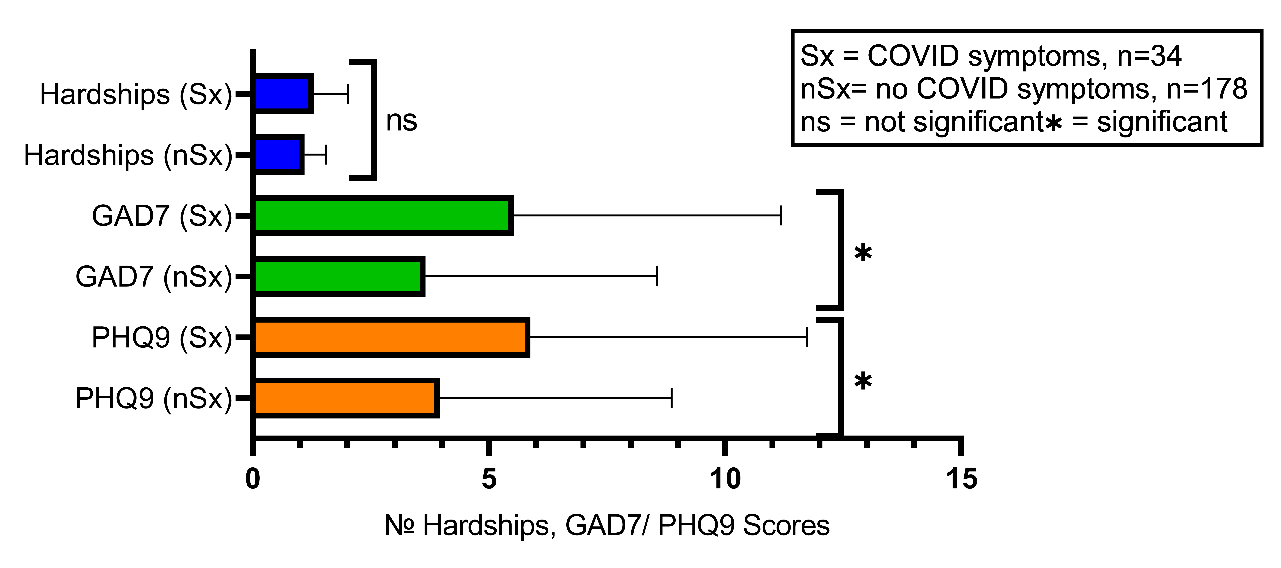
Figure 7: Follow-up #6: Comparison of GAD7, PHQ9, and COVID-19 Related Social and Economic Hardships among Participants with COVID-19 Symptoms vs Participants without COVID-19 Symptoms.
Discussion
There is significant variation in the manifestation of COVID-19 illness and subsequent Long COVID. Some individuals experience more COVID-19 symptoms with various levels of severity8. Although some factors such as low SES7,9-13, age5,7, and medical comorbidities5,7 have been found to influence the occurrence of COVID-19, accurate prognostication is not possible regardless of COVID-19 vaccination status8,11-12. For example, it has been shown that during hospitalization, the most common symptoms were fever, dyspnea, myalgia, cough, and headache. Six months after hospitalization, the most common symptoms were fatigue, dyspnea, myalgia, cough, and headache11. Nevertheless, more than 100 symptoms affecting multiple systems have been reported31. For example, a systematic review suggests individuals with COVID-19 suffer from persistent symptoms: 7% to 42.9% posttraumatic stress disorder, 12% to 30% distress, 6.5% to 42% anxiety, 4.3% to 38.1% depression, 15% to 37.5% dementia/memory loss, 5% to 21% obsessive compulsive disorder, 12% panic attacks, 39% psychiatric morbidity, 0.6% to 19.8% emotional symptoms, 39% to 72% low quality of life, and 1.7% dysphoria31. Other persistent symptoms reported include cardiovascular, pulmonary, respiratory, pain, fatigue, general infection, cognitive, sensory, dermatological, functional, and other symptoms31.
There is a need to identify predictors for short- and long-term COVID-19-related health outcomes, which may inform necessary healthcare services to produce better health outcomes. The variation in COVID-19 and Long COVID symptoms may be partly explained by underlying psychological and/or psychiatric concerns. Preexisting mental illness has been found to be a risk factor for Long COVID development14. Using generalized estimating equation models adjusted for sociodemographic characteristics, health behaviors, and comorbidities, a study conducted by Wang et al, 2022, found that participants with two or more psychological conditions such as worry or perceived stress, had 50% increased risk for Long COVID symptoms14. These authors recommend further exploring the underlying biological mechanisms to better understand mental illness as a risk factor for Long COVID development14. Another study conducted by Hassan et al, 2021, suggests people with mental illness, in particular, people with schizophrenia/psychosis, bipolar disorder, and major depressive disorders, have higher risks of COVID-19 infection, hospitalization, and mortality32. Conversely, a study conducted by Mazza, Palladini, Poletti, and Benedetti, 2022, suggests a peripheral immune- inflammatory response occurs during and after COVID-19 infection, resulting in depression, anxiety, and cognitive impairments33. Given the significant connections between mental and physical illnesses, integrated healthcare approaches may be needed to improve clinical effectiveness and reduce healthcare costs associated with COVID-19 and mental illness comorbidity.
Our findings suggest a significant relationship between anxiety and depression symptoms and COVID-19 symptoms for participants remaining in the study from baseline (66.37%, 53.66%, 44.54%, 37.22%, 35.28%, and 31.69% for follow-ups 1 through 6, respectively). Medical diagnoses and social/economic hardships experienced during the pandemic significantly confound these longitudinal results. Age, sex, and race were not associated with the number of symptoms experienced. Overall, the number of symptoms significantly increase with higher PHQ-9 and GAD-7 scores at every study time point. More symptoms are likely to occur when there is a comorbid mental illness. All data in this study is self-reported, which is a significant limitation. Nevertheless, the use of self-reported outcomes is becoming an integral part of health research studies to maximize the improvement of healthcare quality34-36. An important limitation for this study is the attrition rates over the six follow-ups, with only 31.69% of participants completing the entire study. In addition, the COVIDsmart population is composed of mainly White females. However, other large-scale online studies with no face-to-face interaction have had similar demographics37-38. Effective study recruitment strategies need to be identified for future online studies to capture a more diverse population.
In conclusion, our longitudinal study suggests that the presence of depression and/or anxiety is associated with increased short- and long-term symptoms of COVID-19. Integrated health approaches for COVID-19 and comorbid anxiety and/or depression may be necessary to improve overall health outcomes. Further investigation into the causative mechanisms is warranted.
Data Availability
Data cannot be shared as it was copyrighted by partners for the COVIDsmart study (Eastern Virginia Medical School - Sentara Healthcare Analytics and Delivery Science Institute (HADSI), George Mason University, and Vibrent Health Inc.
Conflict of Interest
Authors have no conflict of interest to report.
Funding Statement
Marketing efforts for recruitment of participants for this study was supported internally by EVMS-Sentara Healthcare Analytics and Delivery Science Institute, George Mason University, and Vibrent Inc – No grants supported this study.
Acknowledgements
We thank the marketing team who utilized several strategies to advertise this study: Katie Maney, Amy Adams, Doug Gardner, Julie Suedmeyer-Buller, and Mary Westbrook.
We thank the team who helped to manage/design this study: Sarah DePerrior, and Joshua Edwards.
We thank the team who supported the Vibrent digital platform: Praduman Jain, Scott Sutherland, Jack Burtch, Dave Klein, Josh Schilling, Alison Young, and Pearson Brown.
We thank Dr. Keith D. Renshaw and Dr. Amira A. Roess for contributing feedback for this manuscript.
References
- Abedi V, Olulana O, Avula V, et al. Racial, economic, and health inequality and COVID-19 infection in the United States. J Racial Ethn Health Disparities. 2021; 8(3): 732-742. https://doi.org/10.1007/s40615-020-00833-4
- Lopez L III, Hart LH III, Katz MH. Racial and ethnic health disparities related to COVID-19. JAMA. 2021; 325(8): 719-720. https://doi.org/10.1001/jama.2020.26443
- Kim EJ, Marrast L, Conigliaro J. COVID-19: Magnifying the effect of health disparities. J Gen Intern 2020; 35(8): 2441-2442. https://doi.org/10.1007/s11606-020-05881-4
- Webb Hooper M, Nápoles AM, Pérez-Stable EJ. COVID-19 and racial/ethnic disparities. JAMA. 2020; 323(24): 2466-2467. doi:10.1001/jama.2020.8598
- Biswas M, Rahaman S, Biswas TK, et al. Association of sex, age, and comorbidities with mortality in COVID-19 patients: A systematic review and meta-analysis. Intervirology. 2020. doi:10.1159/000512592
- Patel JA, Nielsen FBH, Badiani AA, et Poverty, inequality and COVID-19: the forgotten vulnerable. Public Health. 2020; 183: 110-111. doi:10.1016/j.puhe.2020.05.006
- Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals. cdc.gov. Updated February 9, 2023. Accessed 20 February 2023. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html
- Ihle-Hansen H, Berge T, Tveita A, et al. COVID-19: Symptoms, course of illness and use of clinical scoring systems for the first 42 patients admitted to a Norwegian local hospital. Tidsskr Nor Laegeforen (English). 2020; 140(7): 1-12. doi: 4045/timeskr.20.0301
- Nasserie T, Hittle M, Goodman SN. Assessment of the frequency and variety of persistent symptoms among patients with COVID-19: A systematic review. JAMA Netw Open. 2021; 4(5): e2111417. doi: 10.1001/jamanetworkopen.2021.11417
- Ihle-Hansen H, Berge T, Tveita A, et al. COVID-19: Symptoms, course of illness and use of clinical scoring systems for the first 42 patients admitted to a Norwegian local hospital. Tidsskr Nor Laegeforen (English). 2020; 140(7): 1-12. doi: 4045/timeskr.20.0301
- Fernández-de-las-Peñas C, Ortega-Santiago R, Fuensalida-Novo S, et al. Differences in long-COVID symptoms between vaccinated and non-vaccinated (BNT162b2 Vaccine) hospitalized COVID-19 survivors infected with the delta variant. Vaccines. 2022; 10(9): 1481. https://doi.org/10.3390/vaccines10091481
- O'Mahoney LL, Routen A, Gillies C, et The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: A systematic review and meta-analysis. EClinicalMedicine. 2023; 55: 101762. doi: 10.1016/j.eclinm.2022.101762.
- Wisnivesky JP, Govindarajulu U, Bagiella E, et association of vaccination with the persistence of post-COVID symptoms. J Gen Intern Med. 2022; 37(7): 1748-1753. https://doi.org/10.1007/s11606-022-07465-w
- Wang S, Quan L, Chavarro JE, et al. Associations of depression, anxiety, worry, perceived stress, and loneliness prior to infection with risk of post-COVID-19 conditions. JAMA Psychiat. 2022; 79(11): 1081-1091. doi:10.1001/jamapsychiatry.2022.2640
- Raveendran AV, Jayadevan R, Sashidharan Long COVID: An overview [published correction appears in Diabetes Metab Syndr. 2022 May;16(5):102504] [published correction appears in Diabetes Metab Syndr. 2022; 16(12): 102660]. Diabetes Metab Syndr. 2021; 15(3): 869-875. doi:10.1016/j.dsx.2021.04.007.
- Levine GN, Cohen BE, Commodore-Mensah Y, et al. Psychological health, well-being, and the mind-heart-body connection: A scientific statement from the American Heart Association. Circulation. 2021; 143(10): e763-e783. https://doi.org/10.1161/CIR.0000000000000947
- Doherty AM, Gaughran F. The interface of physical and mental health. Soc Psychiatry Psychiatr 2014; 49(5): 673-682. doi:10.1007/s00127-014-0847-7
- Koban L, Gianaros PJ, Kober H, et al. The self in context: Brain systems linking mental and physical Nat Rev Neurosci. 2021; 22: 309-322. doi:https://doi.org/10.1038/s41583-021-00446-8
- Ohrnberger J, Fichera E, Sutton The relationship between physical and mental health: A mediation analysis. Soc Sci Med. 2017; 195: 42-49. https://doi.org/10.1016/j.socscimed.2017.11.008
- Rocks S, Berntson D, Gil-Salmerón A, et al. Cost and effects of integrated care: a systematic literature review and meta-analysis. Eur J Health Econ. 2020; 21: 1211-1221. https://doi.org/10.1007/s10198-020-01217-5
- Bartholmae MM, Roess AA, Renshaw KD, et al. Evaluation of recruitment strategies on inclusiveness of populations at risk for health disparities in the statewide remote online COVIDsmart VJPH. 2022; 7(1): 11-45. Available at: https://commons.lib.jmu.edu/vjph/vol7/iss1/5/
- Vibrent Health Inc. COVIDsmart study explores impacts of pandemic on lives of Virginians. com. Published October 24, 2021. Accessed January 17, 2022. Retrieved from https://www.vibrenthealth.com/COVIDsmart-study-explores-impacts-of-pandemic-on-lives-of-virginians/
- Kroenke K, Spitzer RL, Williams The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001; 16(9): 606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Löwe B, Decker O, Müller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Medical Care. 2008; 46(3): 266-274. doi:10.1097/MLR.0b013e318160d093
- CDC Human Infection with 2019 Novel Coronavirus Case Report Form. Cdc.gov. Accessed 10/7/2020. https://www.cdc.gov/coronavirus/2019-ncov/downloads/pui-form.pdf.
- Ferrer AH, El Korso MN, Breloy A, et al. Robust mean and covariance matrix estimation under heterogeneous mixed-effects model with missing values. Signal Process. 2021; 188: 108195. https://doi.org/10.1016/j.sigpro.2021.108195
- Keselman HJ, Algina J, Kowalchuk RK. The analysis of repeated measures designs: A review. Br J Math Stat Psychol. 2001; 54(1): 1-20. https://doi.org/10.1348/000711001159357
- Mallinckrodt CH, Sanger TM, Dubé S, et al. Assessing and interpreting treatment effects in longitudinal clinical trials with missing data. Biol psychiatry. 2003; 53(8): 754-760. https://doi.org/10.1016/s0006-3223(02)01867-x
- Suryawanshi M. (2019). Mixed Model Repeated Measures (MMRM). Proceedings of the 2019 PHUSE EU: The Clinical Data Science Conference. Retrieved from https://www.lexjansen.com/phuse/2019/as/AS06.pdf
- Siddiqui O. MMRM versus MI in dealing with missing data--a comparison based on 25 NDA data sets. J Biopharm Stat. 2011; 21(3): 423-436. https://doi.org/10.1080/10543401003777995
- Hayes LD, Ingram J, Sculthorpe More than 100 persistent symptoms of SARS-CoV-2 (Long COVID): A scoping review. Front Med. 2021; 8: 750378. doi:10.3389/fmed.2021.750378
- Hassan L, Peek N, Lovell K, et al. Disparities in COVID-19 infection, hospitalization and death in people with schizophrenia, bipolar disorder, and major depressive disorder: a cohort study of the UK Biobank. Mol Psychiatry. 2022; 27: 1248-1255. https://doi.org/10.1038/s41380-021-01344-2
- Mazza MG, Palladini M, Poletti S, et al. Post-COVID-19 depressive symptoms: epidemiology, pathophysiology, and pharmacological CNS Drugs. 2022; 36: 681-702. https://doi.org/10.1007/s40263-022-00931-3
- Coelho A, de Bienassis K, Klazinga N, et al. Mental Health Patient-Reported Outcomes and Experiences Assessment in Portugal. Int J Environ Res Public Health. 2022; 19(18): 11153. doi:10.3390/ijerph191811153
- Heiden BT, Subramanian MP, Nava RG, et al. Routine Collection of Patient-Reported Outcomes in Thoracic Surgery: A Quality Improvement Study. Ann Thorac Surg. 2022; 113(6): 1845-1852. doi:10.1016/j.athoracsur.2021.05.091
- Black N, Burke L, Forrest CB, et al. Patient-reported outcomes: pathways to better health, better services, and better societies. Qual Life Res. 2016; 25(5): 1103-1112. doi:10.1007/s11136-015-1168-3
- Nelson LM, Simard JF, Oluyomi A, et al. US public concerns about the COVID-19 pandemic from results of a survey given via social JAMA Intern Med. 2020; 180(7): 1020-1022. doi:10.1001/jamainternmed.2020.1369
- Singh P, Cumberland WG, Ugarte D, et al. Association between generalized anxiety disorder scores and online activity among US adults during the COVID-19 pandemic: Cross-sectional analysis. JMIR. 2020; 22(9): e21490. doi:10.2196/21490