
Social Anxiety in University Students: Towards an Intentional Life-Skills Based Prevention Model
Hannah Ali*, Steve Joordens
Department of Psychology, University of Toronto Scarborough, Toronto, ON, Canada
Abstract
Research suggests that staying connected with people is very beneficial to our physical and mental well-being. Moreover, a lack of social connection is associated with poor mental and physical health, and lower overall well-being. For individuals with social anxiety, it is particularly difficult to cultivate social connections. Due to the prolonged period of social isolation during the COVID-19 pandemic, research suggests that social anxiety in university students has increased. This study employed a convergent parallel mixed method design and administered a self-reported questionnaire which included quantitative and qualitative questions. The questionnaire was administered to 301 undergraduate students to determine if feelings of social anxiety in students changed during and after the pandemic. This study also analyzed social anxiety levels across racial and ethnocultural demographics and assessed the cultural stigmas and barriers that may prevent students from accessing mental health services. Results from the quantitative analyses showed a significant difference in social anxiety scores before and after the pandemic. However, in our sample, feelings of social anxiety post-pandemic did not differ across race, or income which were our main variables of interest. In addition, there was a positive correlation between social anxiety scores and household income and fear of negative evaluation. The qualitative results showed that important barriers to accessing mental health services include fear of parents learning they are in therapy, cost of mental health services, language barriers, and concern that a therapist would not have cultural sensitivity. This study highlights the need for increased interventions to reduce social anxiety among students, and proposes a preventative approach we refer to as “Life-Skills Training” to address social anxiety.
Introduction
The National Collaborating Centre for Mental Health1 describes social anxiety disorder as a persistent fear of one or more social situations, where the fear is disproportional to the threat posed. They further explain that social anxiety is a common mental-health disorder which impacts most people at some point during their life, with varying levels of symptoms. Individuals with social anxiety typically fear humiliation and negative evaluation from others, and often have poor social skills, thus tending to avoid social situations as a strategy to cope with the fear and anxiety. Many post-secondary school students struggle with social anxiety and as a result, may experience suboptimal personal, educational, occupational and social functioning2. Social anxiety typically develops during childhood or adolescence, and the median age of onset for those who seek treatment later in life is early to mid-teens1. One way of understanding the extent to which social anxiety can impair functioning is to consider Maslow’s Hierarchy of Needs. The ultimate level of Maslow’s hierarchy of needs reflects the human desire to self-actualize3. However, in order to meet this need, one is motivated to first fulfill the more fundamental needs in their hierarchy which include, physiological needs, safety, belonging/love, and esteem needs. According to Maslow, once individuals have physiological and safety needs mostly secured, they become more concerned with the third need in the hierarchy which is social belonging3. This innate and universal need refers to people’s need for interpersonal attachments, and their desire for feelings of belongingness and acceptance from others3,4. This can be satisfied through strong friendships, family bonds, romantic relationships, social groups, etc. Strong social support systems greatly contribute to both physical and mental well-being. These support systems often help individuals to develop better coping skills, attain their goals, and be resilient during crisis5,10. Not satisfying this need and as a result, having poor social connections increases one’s risk of loneliness, depression and anxiety, a prediction supported by research data3,5,6,7.
Research on social anxiety is critical given the importance of social interactions and social connections on overall well-being. Strong social connections are critical to achieving happiness4,5,7,8. As one’s number of friends increases, generally, their mental health improves5,7,9. A study by Epley & Schroeder5, examined interactions between strangers on trains and buses, and found that happiness was higher in participants who connected with strangers compared to those who commuted in solitude. It is also important to note that it is not merely the act of being around others, but also the quality of these connections that benefits one’s health5,7. Many people report that relationships with friends and family makes their life meaningful4. Of course, these benefits only occur when one is able to form and reinforce social connections, which brings us to the issue of social anxiety, as it makes it harder for people to create and maintain social connection. A large portion of the existing research examines social anxiety among university students. Many university students had high levels of social anxiety prior to the COVID-19 pandemic, hereafter referred to as “the pandemic”10,11,12,13,14. Archbell and Coplan15 examined the link between social anxiety in university students, academic communication and student experiences prior to the pandemic. Among the results, social anxiety was negatively correlated to communication with professors, student experiences and socio-emotional functioning14. Research during the pandemic found that young adults were especially vulnerable to the mental health impacts of the pandemic11,13,14,16. The prolonged period of lockdown and social isolation increased the rates of social anxiety among university students7,16. Feelings of social anxiety often persisted once the lockdown was lifted. Despite a desire to interact with people during the lockdown, many reported having more fears after the lockdown was lifted than they did prior to the pandemic, and also reported feeling that their social skills decreased16. Fears included anxiety around setting meetings and interacting with others, and increased feelings of being judged in social contexts7.
Although research shows increased rates of social anxiety during the pandemic, there is a dearth of research investigating the impact of social anxiety on students upon resuming social activities and the return to in-person classes. More research is also needed to better understand the disparities in rates of social anxiety across various demographics, including race and socio-economic status. The existing research suggests that mental health rates are disproportionally higher across racialized groups17,18. This may be due to inequities in accessing mental health services, lack of knowledge and/or trust of the available resources and services, or possible cultural stigma towards mental health services. According to Maslow’s hierarchy of needs, individuals experiencing inequities because of their race or socio-economic status have not fully satisfied the more basic physiological and safety needs. As a result, such individuals may be even less motivated to focus on the need to belong3.
Many individuals who struggle with social anxiety do not seek treatment, despite it being treatable19. This may be due to fear of being judged by others which is one of the characteristics of social anxiety, thus seeking treatment becomes more challenging due to the innate nature of the disorder20. It has been suggested that online therapy may be a suitable option for individuals with anxiety, and especially for those from communities where mental health is strongly stigmatized21,22, since fear of judgment may be particularly strong in these communities.
The objective of this study was to understand the rates of social anxiety among University of Toronto Scarborough (UTSC) students by conducting a questionnaire and analyzing feelings of social anxiety, both during the pandemic and post-pandemic. Feelings of social anxiety was also analyzed across racial and ethnocultural demographics to identify any differences in levels of social anxiety, as well as willingness and comfort to seek out mental health services. Since there are a growing number of studies investigating the efficacy of online therapy, this study explored if this form of therapy is of interest to students. We were especially interested in seeing if it was of interest to students from communities experiencing mental health stigma. This study sought to address the previously mentioned gap in the literature by answering two research questions (1) “has the pandemic contributed to the onset of social anxiety or increased pre-existing feelings of social anxiety among UTSC students during and after the pandemic?” And (2) “does race, ethnocultural identity and/or other demographic factors (i.e., household income, living alone or with others, status as domestic student or international student) impact the rates of social anxiety among UTSC students?” This study had two hypotheses. First, we hypothesized that feelings of social anxiety increased during the pandemic due to the extended period of time with limited social interactions, which can negatively impact students’ social anxiety after the pandemic. Second, we hypothesized that students who are Black, Indigenous and people of colour (BIPOC), may have lower household income or barriers to accessing resources and supports, and as such may experience disproportionate rates of social anxiety.
Methods
Participants
Participants were undergraduate students in the Introduction to Biological and Cognitive Psychology and the Introduction to Clinical, Developmental, Personality and Social Psychology courses at UTSC, and were recruited through the university’s SONA system. Data collection occurred from December 2022 to March 2023. A power analysis was conducted using a medium effect size of Cohen’s d = 0.4 and yielded a minimum sample size of 199 participants to achieve 80% power. A total of 389 students participated in this study. Participants received a course credit as compensation. Once a participant signed up for the study, they were taken directly to the Qualtrics site to access the questionnaire where they read a consent form. Written consent was required before participants began the questionnaire. Students were required to be over 18 years old to participate in this study. To ensure this, students were asked to confirm that they were over 18 years old before starting the questionnaire, however no further questions regarding age was asked. At the end of the study, participants were provided a debrief form, and the researchers’ contact information for questions or comments. Ethics approval for this study was received by the University of Toronto Delegated Ethics Review Committee (protocol number 2022-12).
Missing Data
Before statistical analysis were conducted, the data was cleaned according to the following measures. Of concern with student samples is integrity of the data. Data from students who completed the questionnaire under five minutes were excluded (n = 17) to not compromise the integrity of the conclusions we can draw from responses as this questionnaire is too long to be completed in under five minutes. Thirty participants stated they would not like their data used in the study. Thirteen participants skipped every question on the survey. Responses on reverse ordered questions were assessed. Reverse ordered questions help to provide information on whether or not participants are attending to questions carefully. Due to inconsistencies across reverse ordered and ordered questions, 28 participants were excluded. The total sample included in the analysis was 301 participants.
Study Design and Materials
A convergent parallel mixed methods design was used to conduct an environmental scan of social anxiety levels in students during and after the pandemic. To create the semi-structured questionnaire, four measures which contained both quantitative and qualitative questions were compiled to analyze different components of social anxiety. Questions assessing demographic variables were included to better understand the racial and ethnocultural background of participants, and factors that may contribute to inequity, to understand how inequity may present differently across demographics. Students were asked to complete each question twice; the first round required them to think about their levels of social anxiety during the pandemic, the second round required them to answer the questions as it applied to them at the time they were completing the questionnaire. It is important to note that participants were not asked to disclose any personal information regarding a mental health diagnosis or previous medical history including use of any psychiatric drugs. This was communicated to participants in the questionnaire. None of the questions were mandatory.
In terms of demographic variables, participants were asked questions regarding their race and ethnocultural group and their household income. The income brackets used were adapted from Statistics Canada and is public record23. Students were asked if they were a domestic student, and if they lived alone during the lockdown and at the time of completing the questionnaire.
Assessing inequity helped us understand if feelings toward mental health services and accessing these services are impacted by inequities, barriers, and possible cultural stigma. To assess this, we adapted an inequity questionnaire by Rastogi et al24. Information regarding the reliability and validity of this measure was not provided. The original measure including only open-ended questions. As assessing inequities in rates of mental health across racial groups was one component of our study, we reduced the number of questions included, and adapted some of the questions to be closed-ended. As such, our version of the questionnaire includes open and closed-ended questions (e.g., “reflecting on your cultural values and beliefs, what does therapy or counseling mean to you?”, “would you consider receiving mental health assistance for social anxiety? [yes or no]”).
To assess social anxiety, participants completed the Social Interaction Anxiety Scale (SIAS)25. This is a commonly used measure to assess social anxiety. The validation study for the SIAS resulted in a high test-retest correlation coefficient above 0.90 and high internal consistency (α = .93)26. This scale also has strong construct and discriminant validity and this has been reinforced in the literature27, 28, 29. SIAS is a 20-item self-reported questionnaire with reverse scored items, designed to assess levels of social interaction anxiety (e.g., “I get nervous if I have to speak with someone in authority (teacher, boss, etc.)”, “I find it easy to make friends my own age”, “I feel I’ll say something embarrassing when talking”). Participants rated their responses on a 5-point Likert scale, ranging from “not at all” to “extremely”. A cut-off score of 34 on the SIAS has been used in the literature to identify social anxiety, as such this study also used a cut-off score of 3430,31,32.
Individuals with social anxiety often fear being negatively evaluated, as such this is a significant component of social anxiety. The internal consistency for this measure was high (α = .89), however, sufficient validity scores has not been reported33. Fear of negative evaluation was measured using the 12-item Brief Fear of Negative Evaluation Scale (BFNE)34. Example items include: “I worry about what other people will think of me even when I know it doesn't make any difference” and “I rarely worry about what kind of impression I am making on someone”. This scale is a 5-point Likert scale with responses ranging from “not at all characteristic of me” and “extremely characteristic of me”. A higher score on the BFNE indicates greater fear of negative evaluation.
Statistical Analyses
All quantitative analyses were conducted using Jamovi, an open-source statistics package. We were first interested in comparing the during and post-pandemic SIAS scores of participants. To test this, a paired sample T-test was conducted. Four separate one-way between-subject ANOVA were conducted with post-pandemic SIAS scores as the dependent variable for every test. The four independent variables assessed in each ANOVA were race, income, student status, and living status.
The qualitative questions included two open-ended questions. To analyze these responses the method of constant comparison was used to understand the various cultural stigmas and barriers people experience that prevents them from accessing mental health services. This method is used in grounded theory, and helps to organize data into themes, or groups in a structured way in order to gain knowledge from the responses24.
Results
The results of our research will be discussed across a number of sections. First, we will focus on the demographics representing the participants in our study. We then present a quantitative analysis of the data, followed by a qualitative analysis.
Demographics
As is apparent from Table 1, our sample includes good variability in terms of both Race and Household Income. While most students were domestic students who lived at home both during and after the pandemic, we also had representation of international students.
Table 1: Demographic characteristics of participants.
|
Demographic Variable |
Frequency (n) |
Percent (%) |
|
|
Age |
≥ 18 |
301 |
100% |
|
Race |
White |
35 |
11.63% |
|
Black |
27 |
8.97% |
|
|
East Asian |
78 |
25.91% |
|
|
South Asian |
95 |
31.56% |
|
|
South-East Asian |
15 |
4.98% |
|
|
West Asian |
12 |
3.99% |
|
|
Arab |
8 |
2.66% |
|
|
Latin American |
5 |
1.66% |
|
|
Other |
3 |
1% |
|
|
Mixed |
23 |
7.64% |
|
|
Household Income |
Less than $5,000 |
15 |
4.98% |
|
$5,000 to less than $10,000 |
9 |
2.99% |
|
|
$10,000 to less than $15,000 |
12 |
3.99% |
|
|
$15,000 to less than $20,000 |
7 |
2.33% |
|
|
$20,000 to less than $25,000 |
18 |
5.98% |
|
|
$25,000 to less than $30,000 |
13 |
4.32% |
|
|
$30,000 to less than $40,000 |
20 |
6.64% |
|
|
$40,000 to less than $50,000 |
15 |
4.98% |
|
|
$50,000 to less than $60,000 |
15 |
4.98% |
|
|
$60,000 to less than $70,000 |
15 |
4.98% |
|
|
$70,000 to less than $80,000 |
30 |
9.97% |
|
|
$80,000 to less than $90,000 |
17 |
5.65% |
|
|
$90,000 to less than $100,000 |
29 |
9.63% |
|
|
$100,000 and over |
80 |
16.61% |
|
|
Student status |
Domestic Student |
236 |
78.41% |
|
International Student |
65 |
21.59% |
|
|
Living Status (during COVID-19 lockdown) |
Alone |
20 |
6.64% |
|
With others |
281 |
93.36% |
|
|
Living Status (after COVID-19 lockdown) |
Alone |
38 |
12.62% |
|
With others |
263 |
87.38% |
Quantitative Data
The paired sample T-test yielded significant results, t(300) = 6.27, p < .001, d = .36. Specifically, participants’ SIAS scores were significantly higher during the lockdown portion of the pandemic (Mean = 37.3) compared to the post-pandemic SIAS score (Mean = 33), by a difference of 3.73 bpm (95% CI [0.245, .478]) as depicted in Figure 1. As previously mentioned, this study used 34 as its cut-off, and results indicate social anxiety among students both during and post-pandemic, with social anxiety being worse during the pandemic.
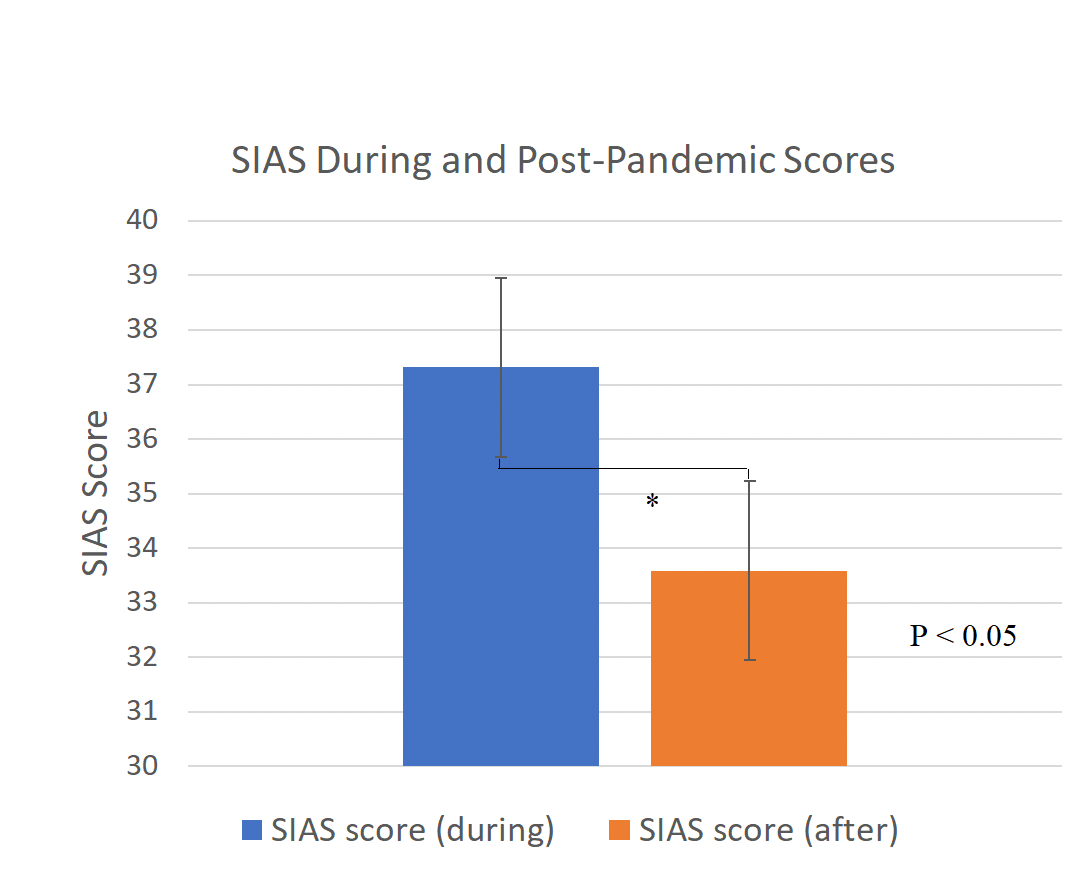
Figure 1: Comparing SIAS Scores during and Post-Pandemic
Data is based on participants SIAS scores for their social anxiety levels during the pandemic and post-pandemic. These scores were compared and levels of social anxiety according to the SIAS was significantly higher during the pandemic compared to post-pandemic.
In order to assess if SIAS post-pandemic scores differed across race, a one-way ANOVA with 10 levels (White, Black, East Asian, South Asian, South-East Asian, West Asian, Arab, Latin American, Other and Mixed) was conducted. The result was not significant, F(9, 29.4) =1.07, p = .415 (Figure 2). A one-way ANOVA analyzing the differences in SIAS post-pandemic scores across income with 14 levels was also conducted (refer to appendix 1 for income levels). This test also yielded non-significant results, F(13, 72.1) = 1.85, p = .05 (Figure 3). A one-way ANOVA measuring SIAS post-pandemic scores was conducted with 2 levels (international and domestic status). The results were not significant, F(1, 108) = .26, p = .61 (Figure 4). Lastly, a one-way ANOVA analysing SIAS post-pandemic scores across two levels (living alone, and living with others post-pandemic) yielded non-significant results, F(1, 50.1) = .07, p = .79 (Figure 5).
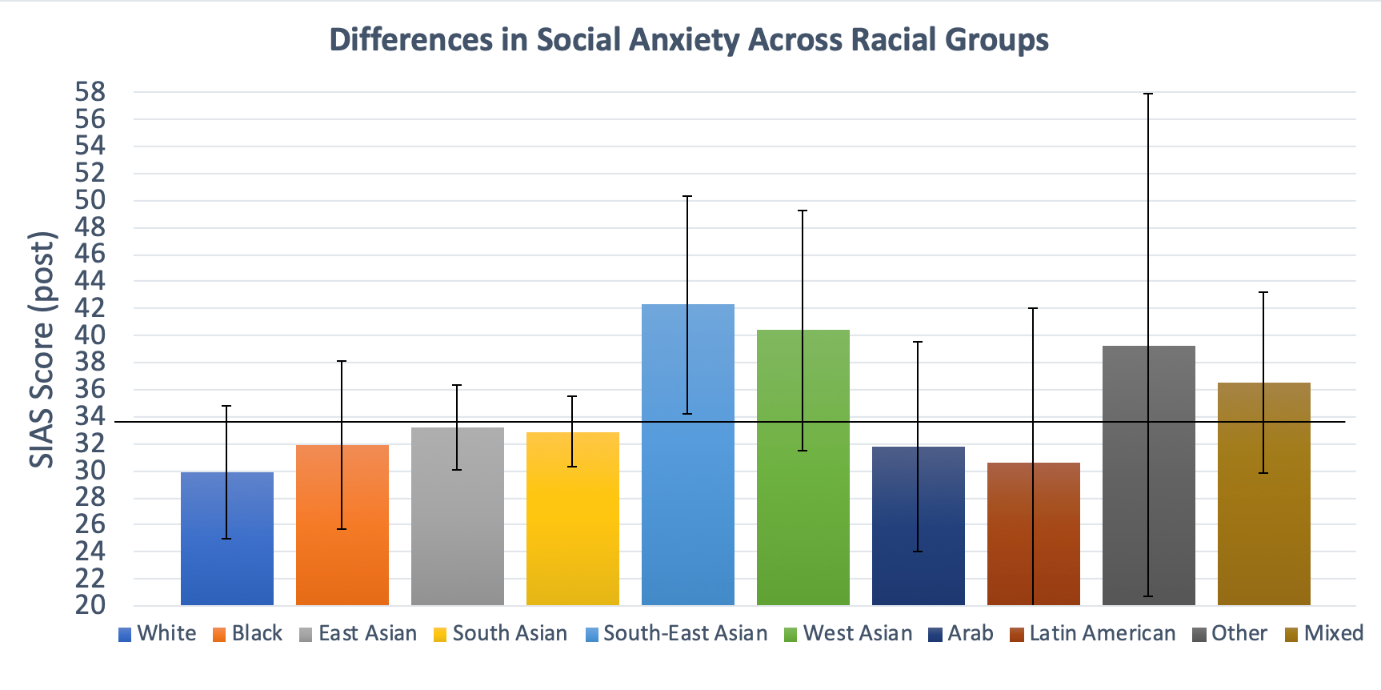
Figure 2: Differences in Social Anxiety Across Racial Groups.
The post-pandemic SIAS scores are compared across the 10 racial groups
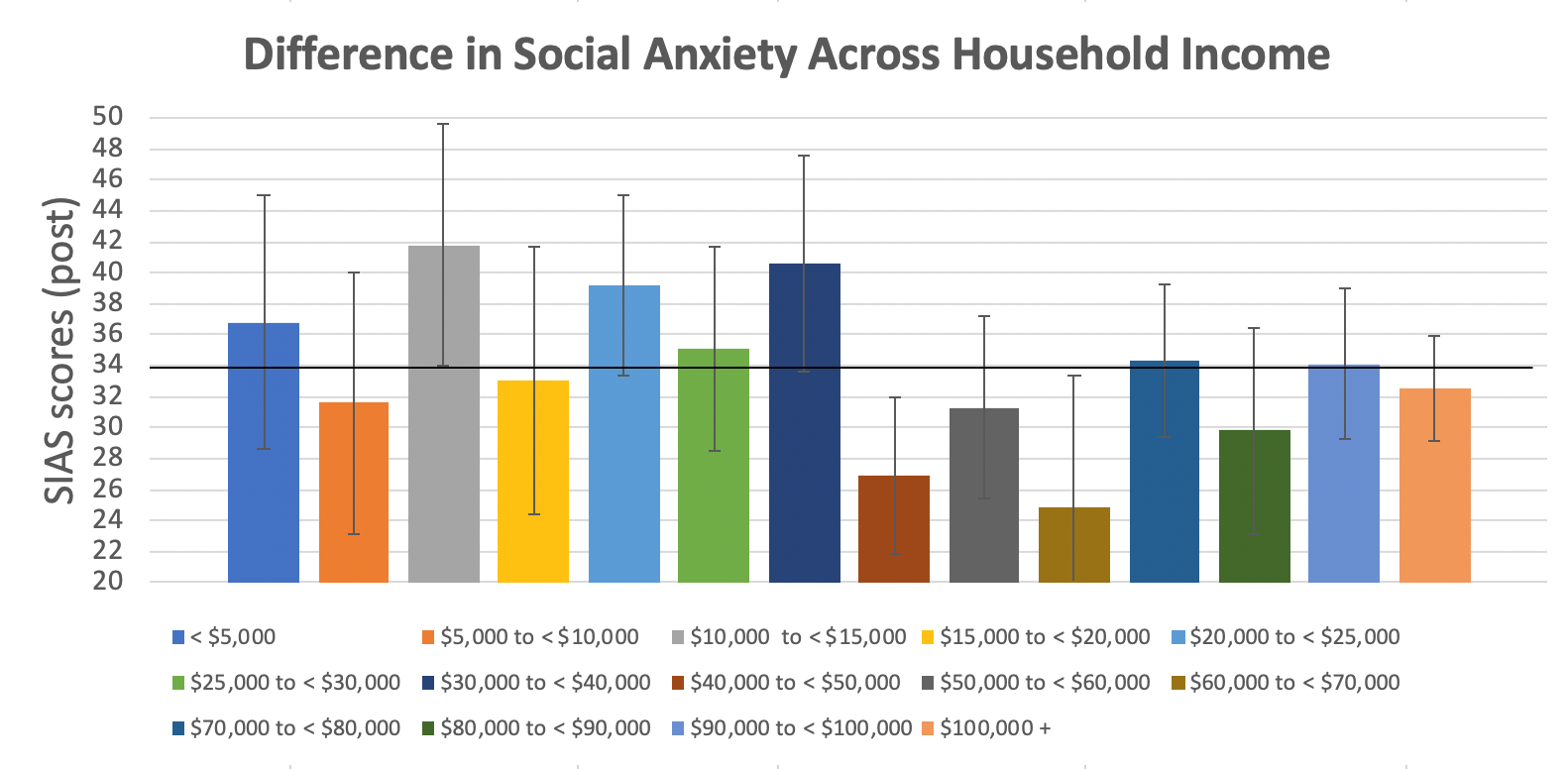
Figure 3: Differences in Social Anxiety Across Household income.
Participants post-pandemic SIAS scores were compared across household income levels.
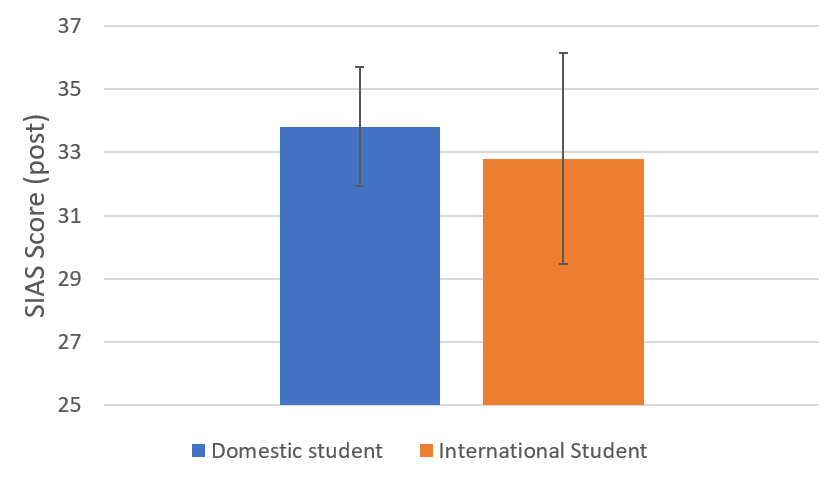
Figure 4: Social Anxiety Across Student Status.
SIAS scores were compared across domestic students and international students. Results did not find a significant difference between these populations.
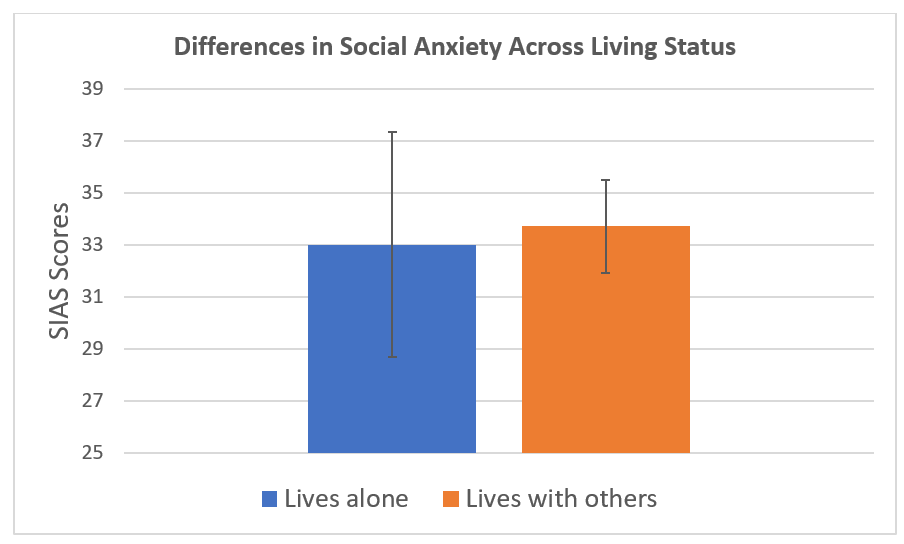
Figure 5: Differences in Social Anxiety Across Living Status.
SIAS post pandemic scores were compared across individuals living alone versus living with others.
A multiple linear regression analyses was conducted to determine if post-pandemic SIAS scores of participants can be predicted by the BFNE post-pandemic scores, race, income, domestic or international student status, and whether they were living alone or with others (post-pandemic). The results showed that 41.1% of the variance in SIAS post-pandemic scores can be explained by the 5 predictors, R2 = .411, F(5, 289) = 42.1, p = < .01. BFNE post-pandemic scores significantly predicted SIAS post-pandemic score. However, race, domestic or international student status, and if the participant were living alone or with others did not significantly predict SIAS post-pandemic scores, see Table 2.
Table 2: Multiple Linear Regression Coefficients.
|
|
|
|
95% Confidence Interval |
|
|
|
95% Confidence Interval |
||
|
Predictor |
Estimate |
SE |
Lower |
Upper |
t |
p |
Stand. Error |
Lower |
Upper |
|
Intercept |
2.688 |
3.462 |
-4.127 |
9.503 |
0.776 |
0.438 |
|
|
|
|
DG 1 (Race) |
0.406 |
0.282 |
-0.149 |
0.961 |
1.439 |
0.151 |
0.066 |
-0.024 |
0.155 |
|
DG 2 (Income) |
-0.421 |
0.153 |
-0.722 |
-0.119 |
-2.744 |
0.006 |
-0.124 |
-0.212 |
-0.035 |
|
DG 3 (Student Status) |
-0.936 |
1.604 |
-4.092 |
2.221 |
-0.583 |
0.560 |
-0.027 |
-0.119 |
0.065 |
|
DG5 (living status) |
-0.361 |
2.009 |
-4.316 |
3.593 |
-0.180 |
0.857 |
-0.009 |
-0.102 |
0.085 |
|
BFNE (post pandemic) |
0.962 |
0.069 |
0.827 |
1.098 |
13.980 |
<0.001 |
0.628 |
0.540 |
0.716 |
The questionnaire also included four multiple choice questions. Participants were asked if they would consider accessing mental health services. Approximately 68% of participants said they would feel comfortable, and 32% said they would not consider accessing services. To understand cultural and social stigmas, participants were asked if they felt that there were cultural or social stigmas about mental health services that impacted the way they engage with mental health services. Almost 74% (n = 22) stated that there are stigmas around accessing mental health services in their culture, and selected which stigmas out of the 4 options exist (see Appendix 2 for this question). Five participants provided additional stigmas which included, assuming individuals who sought mental health services were “crazy” or weak, believing therapy is a waste of time, and believing that social workers will take your children away.
To understand what other factors may prevent participants from accessing mental health services, they were asked if the ethnic background of the mental health provider is an important factor, and 53% reported it was not. Since literature supports provision of online therapy to increase access to mental health services, participants were asked which format of therapy they would feel most comfortable with. Results showed that 68% of participants selected in-person therapy, and this was followed by 13% of participants selecting online therapy. Therapy via telephone was selected the least, with only 3% of participants choosing this option. Twelve percent of participants said they do not know which form of therapy they would prefer and 4% said they would not feel comfortable receiving therapy in any form.
Qualitative Data
All analyses were conducted by one researcher to reduce the possibility of bias into the analyses. The two qualitative questions (in bold), and the themes used to analyze responses are stated below.
Reflecting on your cultural values and beliefs, what does therapy or counseling mean to you?
Responses to this question were sorted according to themes based on participants’ definitions to this question. The five themes were, treatment-based definition, cultural stigma towards mental health services, discussing challenges with a professional, access to services, and no definition provided (Figure 6).
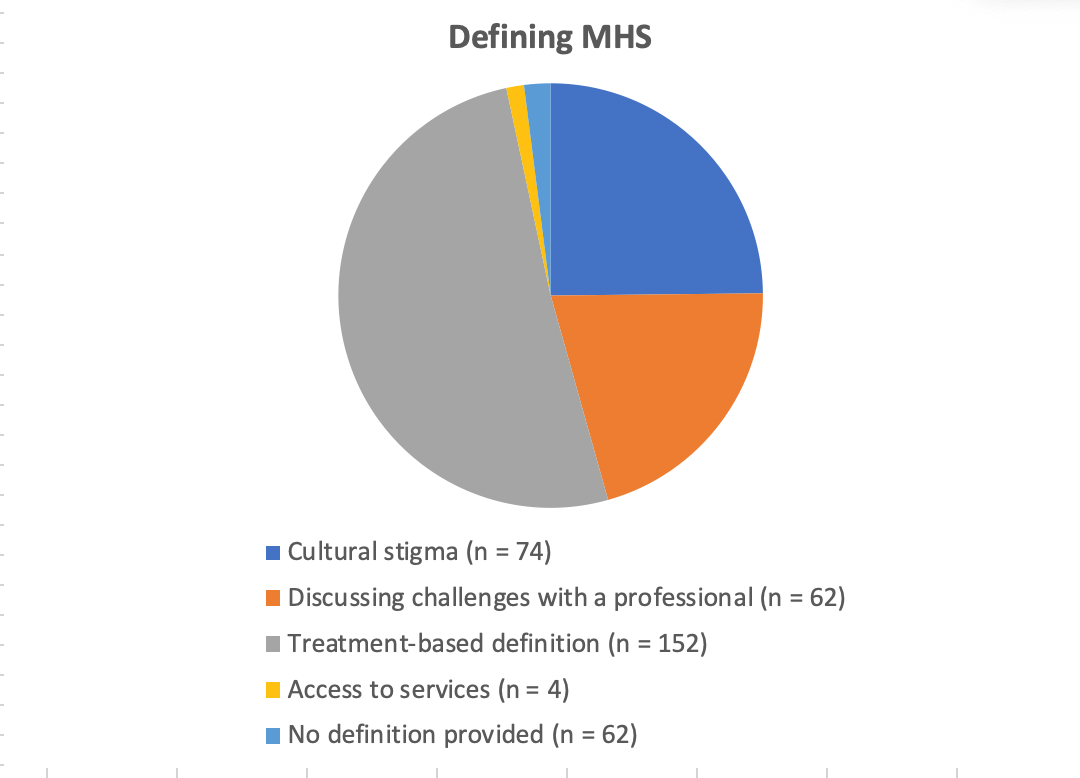
Figure 6: Defining Mental Health Services.
Breakdown of participants’ definitions of therapy according to the five identified themes.
Treatment-based definition: Fifty-one percent of participants defined therapy or counselling by focusing on a medical treatment to address their needs. Four percent of participants stated that it is similar to a physical illness, in that, when you are sick you go to a professional to get better. Three percent of participants defined it as a cure for mental health disorders. Majority described it as a medical treatment that takes time and is challenging, but usually has positive results.
Cultural Stigma towards mental health services: Twenty-five percent of respondents (n = 74) stated that accessing mental health is challenging because of the stigma that exists within their culture. Some stated that therapy is not discussed in a serious matter because mental health issues are not considered “real”. The perception that people are “weak” for needing therapy was common among many cultures. Of the seventy-four participants, 32% identified they would not access therapy for their own needs. Reasons why they would not access therapy included, high cost of a service that may be useless, fear of being thought of as “weak”, or simply not believing in therapy. Thirty-six percent of the seventy-four participants felt that mental health and mental health services are important but are not accepted in their culture. Less than one percent (0.7%) of participants said that although therapy is not accepted in their culture, a person should access care only if they could not find a solution on their own.
Discussing challenges with a professional: Eleven percent of participants defined therapy as opening up to a professional about one’s struggles. Less than one percent (0.3%) of participants defined it as a “deep and relaxing conversation”, others defined it as an outlet, or a way to learn more about yourself and emotional responses. These definitions understood therapy as a way to better express your thoughts and feelings about specific struggles, but also as an important resource to improve one’s overall well-being.
Access to services: Five percent of participants included the importance of equal access to mental health services in their definition. Less than one percent (0.3%) of participants focused on having support from their family to access mental health services.
No definition provided: Eight percent of participants did not answer this question, and Less than one percent (0.3%) of participants said they do not know.
Suppose you needed to seek help with mental health issues, what are some of the challengers or barriers in seeking mental health services?
Barriers experienced by participants to accessing mental health services were divided according to five themes. They were, difficulties obtaining care, sociocultural barriers, individual barriers, and barriers at the family level. Responses where individuals cited there were no barriers, were unsure or did not answer the question were grouped into a fifth theme called “other responses” (Figure 7).
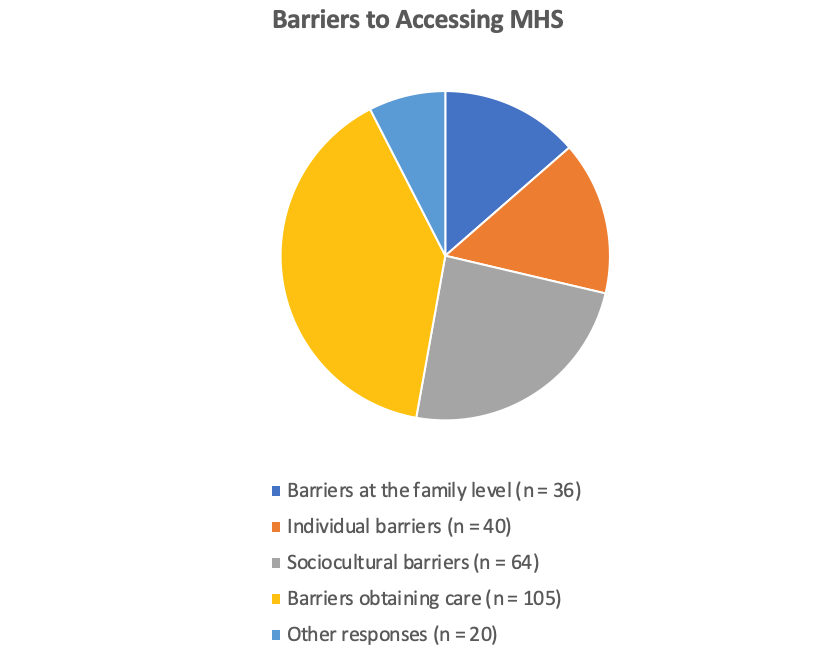
Figure 7: Barriers to Accessing Mental Health Services.
Breakdown of participants responses to barriers to accessing mental health services according to the five identified themes.
Difficulties obtaining care: Six percent of participants reported significant concern that the therapist may not be understanding of, or educated on cultural traditions, customs and practices, and as a result may not apply cultural sensitivity to understand their challenges. Eight percent of participants expanded on this, explaining that they are not confident they would find a therapist who is genuinely interested in helping them and making them feel comfortable enough to open up fully. Finding the mental energy and the time to seek mental health services was cited by 5% of participants as a deterrent. Less than one percent (0.7%) of participants commented that having to travel long distances would prevent them from seeking care.
Twenty percent of participants reported that financial barriers would make it difficult for them to access mental health services. Of this, eight percent of participants commented on the long-wait times as a barrier. Less than one percent (0.3%) of participants spoke about the increased wait-time and challenges of finding a therapist following COVID. Less than one percent (0.7%) of participants reported that a barrier to online therapy post-pandemic is a lack of privacy from those they live with. They stated that the location they used to access free counselling is now virtual, and as such struggled to maintain their therapy. Another participant stated that it is challenging to find mental health services suitable for trans individuals specifically and they do not feel comfortable reliving and retelling their struggles to therapists they feel may not understand.
Sociocultural barriers: Four percent of participants reported that they do not have enough information on what mental health services are, or which services are available to them. Common reason was because mental health services were not discussed much in their cultures as a possible option. Three percent of participants stated that the stigma around mental health, as well as the belief in their culture that mental health is not important serves as barriers to accessing mental health services. Nine percent of participants said that because it is not in their culture to share information with a stranger, they struggle with opening up and as such are not likely to go to therapy.
Less than one percent (0.3%) of participants commented that in their culture, seeking therapy is seen as relying on someone else, which is not desirable as it is better to find ways to help yourself, thus, deterring them from accessing care.
Three percent of participants said they would not access care out of fear that their peers would judge them or look at them differently if they knew. Less than one percent (0.3%) of participants reported that the stigma associated with men who express their feelings is a barrier.
One percent of participants said they would not access mental health services because they do not want to be labeled as “crazy”, “psychopath” or “insane” by society but specifically by people within their culture. Less than one percent (0.7%) of participants said a barrier would be “trying to convince my parents that I am not "crazy" and that [it is] normal [for] every human being to deal with some form of mental health illness and that it is important [to] seek help”. Two percent of participants stated that since English is not their first language, they would not feel comfortable accessing care in English. Less than one percent (0.3%) of participants commented on the difficulty of accessing a translator.
Individual barriers: Twelve percent of participants stated that taking the first step to register for therapy as well as their anxiety or introverted personality would prevent them from seeking care. Many said that the reason they need therapy is also what prevents them from seeking therapy. Less than one percent (0.7%) of participants stated that sometimes individuals do not realize they need help, and that might be a barrier. Less than one percent (0.3%) of participants said their ego would serve as a barrier, commenting:
“Social ego, I like to think of myself as okay or a little above average. Seeking mental health issues would make me feel less of myself even though it does the opposite. I [wasn’t] exposed to [this] kind of help growing up”.
Barriers at the family level: Twelve percent of participants stated that it would make their parents upset to know they are in therapy since they would not understand why they need it or how they could share information with a stranger. Many said their parents would prefer them speaking with a family member, otherwise someone from their church or within their culture. Many reported that the lack of support and encouragement from parents prevented them from wanting to access available services.
One percent of participants stated that they would not want to be a burden on their family, or worry their family by seeking therapy. Four percent of participants said they worry about disclosing their struggles to their family and what their family would think of them for being in therapy.
Other responses: Three percent of participants stated that they do not think there are any barriers to accessing mental health services. Another three percent of participants did not answer this question. Less than one percent (0.3%) of participants indicated they do not know if there are any challenges or barriers.
Discussion
The ability to form strong and meaningful social connections with others has many benefits on one’s health and overall happiness4,5,7,8. Individuals with social anxiety, however, often struggle with forming these social connections. Evidence suggests that the prolonged period of social isolation as a result of the pandemic has increased feelings of social anxiety among university students7,16. Evidence also suggests that there are disparities in rates of mental health disorders17,19. This may be a result of inequities in accessing health care services, lack of knowledge or trust in the available services, and cultural as well as social stigma towards mental health. Increased awareness on these available services and resources are crucial as social anxiety is a treatable disorder despite many people not seeking treatment19. The remainder of our discussions will focus largely on our findings and thoughts on how these findings can be translated into valuable student support practices to reduce social anxiety.
Our study included qualitative and quantitative analyses to best understand feelings of social anxiety among UTSC students during the pandemic and post-pandemic. Results showed that average SIAS scores were higher during the lockdown portion of the pandemic compared to the post-pandemic SIAS scores. These findings support our first hypothesis as we predicted that feelings of social anxiety would be higher during the pandemic. Other studies have also suggested that the pandemic has contributed to an increase in social anxiety in children and adolescents35,36,37,38. Both the during and post-pandemic scores depicted high levels of social anxiety among the participants. While the reduction in social anxiety is noteworthy, the participants’ scores still remain at criterion level that defines someone as “socially anxious”.
We conducted four one-way ANOVAs to assess if post-pandemic social anxiety differed across numerous variables including race, household income, domestic or international student status, and whether or not participants were living alone (post-pandemic). The race groups included in the assessment were retrieved from Statistics Canada. Unfortunately, the racial categories used by Statistics Canada were not consistent in identifying all the racial and ethnocultural groups, this made it challenging to understand the data across the various racial and ethnocultural categories. As such, we amended the categories according to the 10 levels described in this ANOVA. None of the ANOVAs were statistically significant. Thus, our findings did not support our second hypothesis, as social anxiety did not significantly differ across racial and ethnocultural groups among study participants. This differs from research on anxiety across racial groups as many have reported racialized groups to have greater rates of anxiety39,40. However, the results did show that social anxiety was found in almost every race and ethnocultural group. In other words, UTSC students across all racial and ethnocultural groups are experiencing social anxiety.
A multiple linear regression analysis was conducted to see if post-pandemic SIAS scores were predicted by BFNE post-pandemic scores, race, household income, domestic or international student status, and whether participants were living alone or with others (post-pandemic). BFNE scores as well as income were both statistically significant, indicating they do impact social anxiety. Similar findings have been reported in other studies41,42. It has been suggested in the literature that income being a predictor of social anxiety could be because those with a higher household income may have more access to resources42. Eighty students selected over one-hundred thousand dollars as their household income, and this income group had the most responses. Those with a lower household income may have been individuals who had jobs that made them more at risk of COVID-19, for example, students who worked at grocery stores, restaurants etc. As previously mentioned, many individuals with social anxiety often fear being negatively evaluated by others which is why we also assessed fear of negative evaluation. Thus, it is not surprising that it was a predictor of social anxiety scores41. Race, domestic or international student status, and whether participants were living alone or with others were not statistically significant.
To best understand the results of our one-way ANOVA and multiple linear regression analyses, it is important to note that the largest population in the study and across the UofT campuses more broadly, are students from Asia. According to the UofT 2021-2022 enrollment report, the racial and ethnocultural identities of international students showed that 65% of international students are from Asia43. The racial and ethnocultural identities of domestic students were not reported. This results in an underrepresentation in this study of other racial and ethnocultural groups reflective of the general population beyond UofT (i.e., White, Black and Indigenous students). It is important to note that the statistically non-significant results found in this study may not be reflective of feelings of social anxiety across racial groups in the general population. Although race does not seem to affect levels of social anxiety in our sample, the qualitative data shows how race affects one’s understanding of mental health as well as their actions toward accessing mental health services. As such, one’s racial background should not be disregarded when understanding social anxiety and when creating interventions to reduce social anxiety across various populations.
The findings from the quantitative analyses show that students in general are struggling with human interactions, the kind of interactions we know are foundational to mental health and general success in life4,5,7,8. Since university experience is intended to enable students to develop their social skill to achieve success in life, we must move towards a more intentional approach that addresses this directly rather than hoping students will gain these skills organically. That is, when a mental health issue is this widespread, it is time to action preventative approaches rather than being reactive with a treatment approach which simply cannot meet the need44.
Recommendation 1: Given the high levels of social anxiety among the student population, it is imperative that colleges and universities see it as part of their mission to help students overcome their anxieties.
Our qualitative results highlight the profound impact of cultural and societal stigma and lack of knowledge of available mental health services, and the negative consequences this has on one’s likelihood to access these services. These responses align with many of the identified barriers in accessing mental health services reported in previous studies17,45,46. Many reported fears of their parents learning they are in therapy or having to inform their parents that they are struggling. There was also an emphasis on desire for their parents’ approval before seeking these services, and concern of being a burden on their family. This illustrates the different dynamics that occur within collectivist cultures since there is an emphasis on strong family bonds, which can inform decision to access services47. Some participants reported also fearing that their friends would judge them for needing mental health services.
Our findings also highlight some of the challenges some students face when considering treatment options. Participants were hesitant to disclose personal information to a stranger, and some held a fear of being culturally misunderstood. Inadequate information on available mental health services, lack of knowledge of and access to resources on campus and the cost of therapy were also cited as barriers to treatment. Some participants also shared that language barriers prevents them from accessing care. This is a gap that can easily be corrected, by providing translation services and therapists to provide services in the commonly spoken languages at the university48.
Cost was identified as a barrier by sixty-one participants. UTSC Health and Wellness Centre provides mental health services to students, thus this perceived barrier points to the need for increased efforts to spread information on available resources within the university to reduce barriers to accessing mental health services.
Other common concerns included, wait-times, and distance to access services. This is a concern that has greatly increased following the pandemic as the healthcare system continues to be strained due to the health human resource crisis49. Although online therapy would enable participants to access mental health services without traveling, few participants reported that they would be most comfortable with online therapy. This question did not ask participants to provide an explanation, however, a participant describes in a different question that they do not have a private place to conduct their online sessions, thus prefer in-person therapy.
Although ensuring students are aware of the free services provided on campuses is important, this alone does not address this barrier and does not guarantee that these services are accessible to students. Challenges with accessibility as identified by many respondents would require culturally relevant and sensitive care, which is an approach supported in the literature50. This means that the psychotherapists should have ongoing cultural sensitivity training, and be representative of the student demographics at UTSC. Currently, the services are available to students as they need them, but would not address an ongoing difficulty or concerns that leads them to need therapy. As a result, the financial barrier to receiving care still exists as ongoing sessions would not be covered.
Recommendation 2: The optimal approach to helping students overcome their social anxiety is to offer training in creating and maintaining healthy social relationships. By framing this training as a life-skills approach, rather than therapy, resilience can be enhanced without triggering stigmas around mental health.
The previously identified stigmas associated with therapy bring us towards our second recommendation, one that is somewhat complex but from our perspective has great potential. Given the challenges students have in accessing therapy and given how challenging it is for most health and wellness services to meet the demand, it is incumbent for institutions to focus on preventative approaches. Specifically, we want to highlight the possibility of providing support for social anxiety via a “Life-Skills Training” approach that may avoid many of the negative impacts of mental health stigmas. A similar intervention that exists is Social Skills Training, which is a therapeutic approach that helps individuals understand and increase social behaviour51. This intervention has been used to improve social skills in various disorders including social anxiety. The intervention we propose is similar to this, however, our intervention is intended to be used in an academic setting to reduce social anxiety in students.
As described at the outset of this paper, there are great rewards and opportunities available to those with strong social connection skills4,5,7,8,10. As one straightforward and simple example, interviews are won by those who can interact well with interview panels and leave them with good impressions. These are the kind of skills all parents want their children to possess, regardless of cultural or religious background. Thus, one could offer a course or learning experience workshop focused on teaching students the value of social connection skills, then specifically highlighting strategies and tips to aid success. To a large extent these strategies and tips will align with therapeutic approaches to reducing social anxiety52. However, if this approach is rightfully framed as life skills rather than specifically relating to mental health support, this may assist in presenting these necessary skills without the risk of triggering stigmas related to mental health.
Our study also confirmed that social anxiety levels are strongly related to one’s “fear of negative evaluation”. Students tend to vastly overestimate the likelihood of social interactions going poorly, and this fear makes them avoid the kind of practice they need. This is also supported by our finding which showed that the BFNE predicted social anxiety. As such, the approach we suggest would need to directly take on this fear of negative evaluation. As students learn the skills of social connection, they should also be exposed to scaffolded practice using the skills they are learning to minimize the possibility of negative outcomes. For example, early in practice students might be asked to enter into very short, self-terminating virtual conversations with strangers. Early practice partners could be matched to share interests, and perhaps with practice, the length of the conversations, the level of matched interests, and the need to terminate the conversations themselves might be manipulated to increase the challenge as they achieve set targets.
Recommendation 3: The students’ habits related to social anxiety are deeply rooted and strongly connected to their fear of negative evaluation. These must be replaced by more adaptive habits and beliefs, a process only possible if knowledge related to social connection and social anxiety is augmented by clear tips and strategies and many opportunities to safely practice using these skills. Thus, the practice component of the intervention must be thought out deeply to provide a ladder of success as students social connection skills grow.
We imagine an intervention made available to students very early in their tenure, optimally at the start of their first semester. The intervention would be focused on enhancing social connection skills and would include both theory with scaffolded practice designed to support successful learning. This intervention would be framed as what it truly is, an opportunity for students to gain the ability to effectively interact with other human beings, even those they are meeting for the first time. We refer to this as a life-skills approach to address social anxiety. With this approach, students will also be taught skills that they can use in various social and professional settings. Specifically, students will be taught skills such as interviewing, conducting presentations, networking, writing emails, communicating through various modalities (i.e. in-person, electronically, etc.) and with different audiences (i.e., peers, professors, other educators, colleagues, employers, etc.). This approach provides individuals with the skills that therapy aims to develop but reduces the risk of stigma when accessing therapy.
The grander hope, of course, is that this training will help students enhance their social connections and as a result, this should make them more resilient to the stresses of university life. The aim is that treatment itself, as provided by health and wellness centres, will be needed by fewer students. Any resources invested in setting up and providing the social connection training would be offset by the reduced demand for treatment. In addition, our students would carry these skills with them, providing them with improved physical and mental health throughout their lives.
Study Limitations
To understand feelings of social anxiety during and post-pandemic, it was critical that participants reflect on how they felt during the lockdown and answer each question accordingly. However, this was a study limitation as participants relied on memory of their symptoms approximately two years prior. Although this may have impacted the reliability of participants’ responses, we felt this was nevertheless important to include to test our hypothesis.
We amended the race and ethnocultural groups from Statistics Canada to align with the 10 ANOVA levels described in this study. While our amendment did not change the race or ethnocultural group of any participant, there was a bit of subjectivity introduced to the study by way of the amendment. The reason for the amendment was to increase our ability to make comparisons across the different race and ethnocultural categories as the original breakdown made this challenging. The racial and ethnocultural demographics of UTSC students do not reflect the demographics of the general population which is a limitation of our sample population and not representative of the study population. Consequently, our findings which suggest no correlation between racial and ethnocultural identity and experiences of social anxiety cannot be transferred to the general population. The racial and ethnocultural data for UTSC students specifically is not available. However, looking at the racial and ethnocultural data of our study participants, we note that South Asian and East Asian students make up over 58% of UTSC students (32% and 26% respectively), with only 9% identifying as Black, 12% as White, and a much smaller representation across other racial categories, with none identifying as Indigenous. Numerous other data show that Black and Indigenous communities are more likely to experience challenges in accessing necessary healthcare services, including mental health services; and when they do, they are more likely to experience bias and discrimination in care leading to disparities in health outcomes18,45. Further research is required to determine if there is indeed an association between racial and ethnocultural identity and rates of social anxiety, to ensure that appropriate, culturally relevant and accessible services are provided to communities that may be experiencing disparities.
Despite the limitations noted, the recommendations proposed can create or strengthen preventative approach to addressing social anxiety in students. To restate, the recommendations are:
- Given the high levels of social anxiety among the student population, it is imperative that colleges and universities see it as part of their mission to help students overcome their anxieties.
- The optimal approach to helping students overcome their social anxiety is to offer training in creating and maintaining healthy social relationships. By framing this training as a life-skills approach, rather than therapy, resilience can be enhanced without triggering stigmas around mental health.
- The students’ habits related to social anxiety are deeply rooted and strongly connected to their fear of negative evaluation. These must be replaced by more adaptive habits and beliefs, a process only possible if knowledge related to social connection and social anxiety is augmented by clear tips and strategies and many opportunities to safely practice using these skills. Thus, the practice component of the intervention must be thought out deeply to provide a ladder of success as students social connection skills grow.
Conclusion
To understand the extent to which students are struggling from social anxiety post pandemic, this study assessed changes in feelings of social anxiety among UTSC students during and post pandemic. The findings provide evidence for social anxiety in students, and indicates that social anxiety scores were significantly higher during the pandemic compared to post pandemic. Although we predicted that social anxiety scores would differ across racial demographics, we did not find any differences across racial groups within UTSC. Students most commonly defined therapy and counselling as seeking professional help to treat disorders or as an opportunity to open up to a professional about one's challenges. Many barriers were identified as preventing students from accessing mental health services. Common barriers included having to share one’s struggles with family members, socio-cultural stigmas, individual barriers, and difficulties accessing care. In response to the many barriers identified, a life-skills approach to address social anxiety was proposed as a way to increase students’ social skills whilst minimizing the risk of stigma.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Social anxiety disorder: recognition, assessment and treatment. Leicester (UK): British Psychological Society UK; 2013.
- Hakami RM, Mahfouz MS, Adawi AM, et al. Social anxiety disorder and its impact in undergraduate students at Jazan University, Saudi Arabia. Mental illness. 2018.
- Taormina RJ, Gao JH. Maslow and the Motivation Hierarchy: Measuring Satisfaction of the Needs. The American journal of psychology. 2013; 126(2): 155-77.
- Baumeister RF, Vohs KD, Aaker JL, et al. Some key differences between a happy life and a meaningful life. The journal of positive psychology. 2013; 8(6): 505-16.
- Epley N, Schroeder J. Mistakenly Seeking Solitude. Journal of experimental psychology General. 2014; 143(5): 1980-99.
- Borg ME, Willoughby T. Affinity for Solitude and Motivations for Spending Time Alone Among Early and Mid- Adolescents. Journal of youth and adolescence. 2022; 51(1): 156-68.
- Martino J, Pegg J, Frates EP. The Connection Prescription: Using the Power of Social Interactions and the Deep Desire for Connectedness to Empower Health and Wellness. American Journal of Lifestyle Medicine. 2017; 11(6): 466-75.
- Bartolini S, Bilancini E, Pugno M. Did the Decline in Social Connections Depress Americans’ Happiness? Social indicators research. 2013; 110(3): 1033-59.
- Seppala E, Rossomando T, Doty JR. Social Connection and Compassion: Important Predictors of Health and Well-Being. Social research. 2013; 80(2): 411-30.
- Kim H, Rackoff GN, Fitzsimmons-Craft EE, et al. College Mental Health Before and During the COVID-19 Pandemic: Results From a Nationwide Survey. Cognitive therapy and research. 2022; 46(1): 1-10.
- Kulcar V, Bork-Hüffer T, Schneider AM. Getting Through the Crisis Together: Do Friendships Contribute to University Students’ Resilience During the COVID-19 Pandemic? Frontiers in psychology. 2022; 13: 880646-880646.
- Morrison AS, Heimberg RG. Social Anxiety and Social Anxiety Disorder. Annual review of clinical psychology. 2013; 9(1): 249-74.
- Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Globalization and health. 2020; 16(1): 57-57.
- Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. Journal of affective disorders. 2020; 277: 55-64.
- Archbell KA, Coplan RJ. Too Anxious to Talk: Social Anxiety, Academic Communication, and Students’ Experiences in Higher Education. Journal of emotional and behavioral disorders. 2022; 30(4): 273-86.
- Liyanage S, Saqib K, Khan AF, et al. Prevalence of Anxiety in University Students during the COVID-19 Pandemic: A Systematic Review. International journal of environmental research and public health. 2021; 19(1): 62.
- Hofmann SG, Anu Asnaani MA, Hinton DE. Cultural aspects in social anxiety and social anxiety disorder. Depression and anxiety. 2010; 27(12): 1117-27.
- McGuire TG, Miranda J. Racial and Ethnic Disparities in Mental Health Care: Evidence and Policy Implications. Health affairs (Project Hope). 2008; 27(2): 393-403.
- Zamorski MA, Ward RK. Social anxiety disorder: common, disabling, and treatable. Journal of the American Board of Family Medicine. 2000; 13(4): 251-60.
- Olfson M, Guardino M, Struening E, et al. Barriers to the Treatment of Social Anxiety. The American journal of psychiatry. 2000; 157(4): 521-7.
- Austin DW, Bhola P, Tebble C, et al. Preferences for Online Mental Health Services Among Australian and Indian Samples: A Cross-Cultural Comparison. Psychological studies. 2018; 63(4): 376-83.
- Rajgopal A, Li CR, Shah S, et al. The use of telehealth to overcome barriers to mental health services faced by young people from Afro-Caribbean backgrounds in England during the COVID-19 pandemic. Journal of Global Health. 2021; 11: 03040. https://doi.org/10.7189/jogh.11.03040.
- 2016 Census of Population questions, long form (National Household Survey) [internet]. Statistics Canada; 2016 [cited 2022 Oct 7]. Available from: https://www12.statcan.gc.ca/nhs-enm/2016/ref/questionnaires/questions-eng.cfm
- Rastogi M, Massey-Hastings N, Wieling E. Barriers to Seeking Mental Health Services in the Latino/a Community: A Qualitative Analysis. Journal of systemic therapies. 2012; 31(4): 1-17.
- Mattick RP, Clarke JC. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour research and therapy. 1998; 36(4): 455-70.
- Tavoli A, Melyani M, Bakhtiari M, et al. The Brief Fear of Negative Evaluation Scale (BFNE): translation and validation study of the Iranian version. BMC psychiatry. 2009; 9(1): 42-42.
- Heimberg RG, Mueller GP, Holt CS, et al. Assessment of anxiety in social interaction and being observed by others: The social interaction anxiety scale and the Social Phobia Scale. Behavior therapy. 1992; 23(1): 53-73.
- de Beurs E, Tielen D, Wollmann L. The Dutch Social Interaction Anxiety Scale and the Social Phobia Scale: Reliability, Validity, and Clinical Utility. Psychiatry journal. 2014; 2014: 1-9.
- Carleton RN, Thibodeau MA, Weeks JW, et al. Comparing Short Forms of the Social Interaction Anxiety Scale and the Social Phobia Scale. Psychological assessment. 2014; 26(4): 1116-26.
- Brown EJ, Turovsky J, Heimberg RG, et al. Validation of the Social Interaction Anxiety Scale and the Social Phobia Scale Across the Anxiety Disorders. Psychological assessment. 1997; 9(1): 21-7.
- Heimberg RG, Mueller GP, Holt CS, et al. Assessment of anxiety in social interaction and being observed by others: The social interaction anxiety scale and the Social Phobia Scale. Behavior therapy. 1992; 23(1): 53-73.
- Rodebaugh TL, Woods CM, Heimberg RG, et al. The Factor Structure and Screening Utility of the Social Interaction Anxiety Scale. Psychological assessment. 2006; 18(2): 231-7.
- Çam S, Yerlikaya EE. A Study on the Construct Validity of the Brief Fear of Negative Evaluation Scale (BFNE). European Journal of Educational Sciences. 2020; 7(4): 40-56.
- Leary MR. A Brief Version of the Fear of Negative Evaluation Scale. Personality & social psychology bulletin. 1983; 9(3): 371-5.
- Tekin U. Evaluation of Psychosocial Symptoms in Adolescents During the COVID-19 Pandemic in Turkey by Comparing Them with the Pre-pandemic Situation and Its Relationship with Quality of Life. Medical Journal of Bakirkoy. 2022; 18: 348-355.
- Charmaraman L, Lynch AD, Richer AM, et al. Examining early adolescent positive and negative social technology behaviors and well-being during the COVID-19 pandemic. Technol Mind Behav. 2022.
- Zhu S, Zhuang Y, Lee P, et al. The changes of suicidal ideation status among young people in Hong Kong during COVID-19: A longitudinal survey. Journal of affective disorders. 2021; 294: 151-8.
- Kindred R, Bates GW. The Influence of the COVID-19 Pandemic on Social Anxiety: A Systematic Review. International journal of environmental research and public health. 2023; 20(3): 2362.
- Jacobs M, Burch AE. Anxiety during the Pandemic: Racial and ethnic differences in the trajectory of fear. Journal of affective disorders. 2021; 292: 58-66.
- Thomeer MB, Moody MD, Yahirun J. Racial and Ethnic Disparities in Mental Health and Mental Health Care During The COVID-19 Pandemic. Journal of racial and ethnic health disparities. 2023; 10(2): 961-76.
- Fredrick JW, Luebbe AM. Prospective Associations Between Fears of Negative Evaluation, Fears of Positive Evaluation, and Social Anxiety Symptoms in Adolescence. Child psychiatry and human development. 2022: 1-11.
- Vine M, Stoep AV, Bell J, et al. Associations Between Household and Neighborhood Income and Anxiety Symptoms in Young Adolescents. Depression and anxiety. 2012; 29(9): 824-32.
- Enrollment report 2021-22 [internet]. University of Toronto Planning and Budget Office; 2022 [cited 2023 Feb 23]. 54 p. Available from: https://planningandbudget.utoronto.ca/wp-content/uploads/2022/04/22-23EnrolmentReport_NMFinal-for-GC.pdf
- Barrett P, Cooper M. Chapter 11 - Prevention and Early Intervention of Social Anxiety Disorder. In: Social Anxiety. Third Edition. Elsevier Inc; 2014. p. 311–30.
- Goetz CJ, Mushquash CJ, Maranzan KA. An Integrative Review of Barriers and Facilitators Associated with Mental Health Help Seeking Among Indigenous Populations. Psychiatric services (Washington, DC). 2023; 74(3): 272-81.
- Lesure-Lester GE, King N. Racial-Ethnic Differences in Social Anxiety Among College Students. Journal of college student retention: Research, theory & practice. 2005; 6(3): 359-367.
- Gopalkrishnan N. Cultural Diversity and Mental Health: Considerations for Policy and Practice. Frontiers in public health. 2018; 6: 179-179.
- Al Shamsi H, Al Mashrafi S, Al Kalbani T, et al. Implications of Language Barriers for Healthcare: A Systematic Review. Oman medical journal. 2020; 35(2): 1-7.
- Kourgiantakis T, Markoulakis R, Lee E, et al. Access to mental health and addiction services for youth and their families in Ontario: perspectives of parents, youth, and service providers. International journal of mental health systems. 2023; 17(1): 4-4.
- Meyer OL, Zane N. The Influence of Race and Ethnicity in Clients’ Experiences of Mental Health Treatment. Journal of community psychology. 2013; 41(7): 884-901.
- Kolakowsky-Hayner S.A. Social Skills Training. Encyclopedia of Clinical Neuropsychology. 2011: 2314-2315.
- Olivares-Olivares PJ, Ortiz-González PF, Olivares J. Role of social skills training in adolescents with social anxiety disorder. International journal of clinical and health psychology. 2019; 19(1): 41-8.
Appendix
Appendix 1: Demographic Questions
- Select the following racial/ethnocultural group(s) you identify with
a) First Nations, Metis, Inuk (Inuit)
b) White
c) South Asian (e.g., East Indian, Pakistani, Sri Lankan)
d) Chinese
e) Black (if selected, skip logic)
- African
- African American
- African Canadian
- African Caribbean
- African Nova Scotian
f) Filipino
g) Arab
h) Latin American
i) Southeast Asian (e.g., Vietnamese, Cambodian, Laotian, Thai)
j) West Asian (e.g., Iranian, Afghan)
k) Korean
l) Japanese
m) Other group — specify:
- What is your total household income?
a) Less than $5,000
b) $5,000 to less than $10,000
c) $10,000 to less than $15,000
d) $15,000 to less than $20,000
e) $20,000 to less than $25,000
f) $25,000 to less than $30,000
g) $30,000 to less than $40,000
h) $40,000 to less than $50,000
i) $50,000 to less than $60,000
j) $60,000 to less than $70,000
k) $70,000 to less than $80,000
l) $80,000 to less than $90,000
m) $90,000 to less than $100,000
n) $100,000 and over
- Are you a domestic student?
a) Yes, I am
b) No, I am an international student
- During the COVID-19 Pandemic, did you live alone?
a) Yes, I live alone
b) No, I live with others
- Do you currently live alone?
a) Yes, I live alone
b) No, I live with others
Appendix 2: Inequity Questions
- Reflecting on your cultural values and beliefs, what does therapy or counseling mean to you?
- Would you consider receiving mental health assistance for social anxiety?
a) Yes
b) No
- Do you think there is any type of cultural or social stigmas in your culture associated with receiving mental health services?
a) Yes
- Cultural taboo around sharing personal health information, including mental health with strangers
- Concern of what others would think
- Disbelief that mental health is a real ailment
- Preference to seek spiritual/religious healing versus psychological treatment
- Other
b) No, there are no cultural or social stigmas in my culture associated with receiving mental health services
- Would the racial or ethnic background of the mental health provider be an important factor for you?
a) Yes
b) No
c) I don’t know
- Suppose you needed to seek help with mental health issues, what are some of the challengers or barriers in seeking mental health services.
- What format would you feel most comfortable receiving mental health services in ?
a) In person
b) Online
c) Telephone only
d) I don’t know
e) I would not feel comfortable receiving any kind of mental health service
Appendix 3: Social Interaction Anxiety Scale (R indicates reverse ordered questions)
- I get nervous if I have to speak with someone in authority (teacher, boss, etc.)
- I have difficulty making eye contact with others
- I become tense if I have to talk about myself or my feelings
- I find it difficult to mix comfortably with the people I work with
- I find it easy to make friends my own age (R)
- I tense up if I meet an acquaintance in the street
- When mixing socially, I am uncomfortable
- I feel tense if I am alone with just one other person
- I am at ease meeting people at parties, etc (R)
- I have difficulty talking with other people
- I find it easy to think of things to talk about (R)
- I worry about expressing myself in case I appear awkward
- I find it difficult to disagree with another’s point of view
- I have difficulty talking to attractive persons of the opposite sex
- I find myself worrying that I won’t know what to say in social situations
- I am nervous mixing with people I don’t know well
- I feel I’ll say something embarrassing when talking
- When mixing in a group, I find myself worrying I will be ignored
- I am tense mixing in a group
- I am unsure whether to greet someone I know only slightly
Appendix 4: Brief Fear of Negative Evaluation (R indicates reverse ordered questions)
- I worry about what other people will think of me even when I know it doesn't make any difference
- I am unconcerned even if I know people are forming an unfavorable impression of me (R)
- I am frequently afraid of other people noticing my shortcomings
- I rarely worry about what kind of impression I am making on someone (R)
- I am afraid others will not approve of me
- I am afraid that people will find fault with me
- Other people's opinions of me do not bother me (R)
- When I am talking to someone, I worry about what they may be thinking about me
- I am usually worried about what kind of impression I make
- If I know someone is judging me, it has little effect on me (R)
- Sometimes I think I am too concerned with what other people think of me
- I often worry that I will say or do the wrong things