
Generalized Anxiety Disorder and Depression Associated with Developmental Prosopagnosia: A Case Report
Kaishi Imatani1, Takeshi Inoue2*, Yuji Oto1, Tasuku Kitajima2, Ryoko Otani2, Satoshi F Nakashima3, So Kanazawa4, Masami K. Yamaguchi5, Ryoichi Sakuta2, Tomoyo Matsubara1
1Department of Pediatrics, Dokkyo Medical University Saitama Medical Center, Koshigaya, Saitama, Japan
2Child Development and Psychosomatic Medicine Center, Dokkyo Medical University Saitama Medical Center, Koshigaya, Saitama, Japan
3Department of Psychological Sciences, University of Human Environments, Okazaki, Aichi, Japan
4Department of Psychology, Japan Women’s University, Kawasaki, Kanagawa, Japan
5Department of Psychology, Chuo University, Hachioji, Tokyo, Japan
Abstract
Developmental prosopagnosia is a disorder of facial recognition that begins during early childhood in the absence of acquired central nervous system disease. We report the case of a 15-year-old female with developmental prosopagnosia as measured by the 20-item Prosopagnosia Index and Cambridge Face Memory Test who ultimately developed generalized anxiety disorder and depression despite relatively normal social and psychological function during early childhood. In elementary school, the case patient adapted by learning alternative ways to identify others, such as by clothing and hairstyle, but this became more difficult in junior high school due to the requirement for school uniforms and regulations on hairstyle. This difficulty in turn led to interpersonal problems that ultimately resulted in symptoms of generalized anxiety disorder and depression, such as headache and sleep dysfunction. People with developmental prosopagnosia are generally prone to having depressed and anxious feelings. However, to the best of our knowledge, this is the first case report of anxiety disorder or depression related to developmental prosopagnosia. This comorbidity may be relatively common, especially in ethnically homogeneous countries with strict school regulations on personal appearance such as Japan.
Introduction
Prosopagnosia is a type of agnosia characterized by difficulty recognizing known and new faces due to neurological dysfunction, particularly in the fusiform gyrus of the inferior temporal lobe1. The term prosopagnosia was first used by Bodamer in 1947 in a detailed description of two patients2, and in the years since, many cases have been reported. Most cases reported initially were of acquired prosopagnosia caused by central nervous system (CNS) diseases such as head trauma and cerebral infarction, but in 1976, McConachie reported the case of AB, a young female with no history of head trauma or other CNS diseases and no intellectual disability who could not recognize faces except those encountered frequently3. As a result of this and similar case reports, the concept of developmental prosopagnosia was proposed in 20061.
Developmental prosopagnosia begins in early childhood and continues throughout life. However, it is not listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)4 and there are no standard diagnostic criteria despite recent reports that prevalence is as high as 2%–2.9% of the general population5. It has been reported that the fusiform gyrus is smaller, and exhibits altered activity patterns in patients with developmental prosopagnosia compared to normally developed individuals6, while the possible influence of other brain regions or networks remains controversial.
In many situations, individuals with developmental prosopagnosia can adapt by learning alternative ways to identify others, such as by their clothing, hairstyle, voice, and other (non-facial) characteristics7. While Davis et al. reported an association between prosopagnosia and social anxiety8. Pressl et al.9 revealed that developmental prosopagnosia coexists with certain comorbid conditions, such as personality disorders, depression, and anxiety, using a large database of more than 7.5 million de-identified electronic health records from patients in New York City. Consequently, patients with developmental prosopagnosia may develop a tendency to avoid personal interactions with others, experience impairment in social functioning, including difficulties in schooling and work, and may exhibit associated mood disorders.
However, we have not found any case reports detailing the temporal relationship between the emergence of face recognition difficulties and psychiatric comorbidities related to developmental prosopagnosia. Herein, we report a case of developmental prosopagnosia associated with generalized anxiety disorder and depression. The reporting of this case was approved by the Ethical Committee of the Dokkyo Medical University Saitama Medical Center (No.22020) and informed consent was obtained.
Case
A 15-year-old female was referred to our hospital with chief complaints of sleep disturbance and headache. Perinatal history, past medical history, and family history were unremarkable. No gross motor, fine motor, or language delays were noted in infancy or during medical checkups at 1.5 and 3 years of age. There were also no problems with social development, such as eye contact and joint attention, during preschool, kindergarten, and elementary school. In addition, interpersonal relationships were normal according to teachers’ reports. However, functional headaches including migraine and tension-type headache, began after entering junior high school and treatment by a local doctor resulted in no clinically significant improvement. In addition to functional headache, fatigue and sleep disorder appeared which led to frequent school absenteeism. In the fall of second-year junior high school, melatonin was prescribed for sleep, but symptoms did not improve, and the patient was referred to our hospital that winter.
At first consultation, the patient was instructed on sleep hygiene and lifestyle, but again no improvement was observed. In June of third-year junior high school, the patient was admitted to our hospital for a thorough examination and treatment of current symptoms, including sleep disorder and headache. Physical examination on admission revealed no apparent abnormalities. During the medical interview, however, the patient answered with downcast eyes and sometimes burst into tears, indicating that she was in a depressed mood. Clinical and neuropsychological assessments were then administered, including the Depression Self-Rating Scale for Children (DSRS-C), Spence Children’s Anxiety Scale, Wechsler Intelligence Scale for Children-Fourth Edition (WISC-IV), and Mini-International Neuropsychiatric Interview-KID (MINI-KID) (Table 1). During these examinations, the tester was told that the patient was having trouble distinguishing the faces of nurses working on the ward; therefore, a detailed interview regarding face recognition was conducted, during which the patient revealed the following: “I cannot remember people’s faces but recognize them by their voices and moods,” “I cannot recognize even my friends when their hairstyle changes,” “I can confidently call people with distinctive body shapes,” “In elementary school, I could remember names but not faces and had difficulty recognizing my friends,” “When I was in the lower grades, I used to play with many different friends and groups, but in the upper grades, I only played with certain friends or groups,” “In junior high school, I could not distinguish my friends because they had similar uniforms and hairstyles,” and “It was difficult for me to call out to them, and it affected my difficulty in going to school.”
Based on these statements, we suspected developmental prosopagnosia and administered the 20-item Prosopagnosia Index (PI-20)10,11 and Cambridge Face Memory Test (CFMT)12. The total score on the PI-20 (81 out of 100 or 2.32 standard deviations [SDs] above the norm) (Table 1) suggested developmental prosopagnosia. On the CFMT as well, the score of 15 points on Section 1 (6.41 SD below the norm) suggested developmental prosopagnosia. In contrast, scores were closer to the norm on Section 2 (19 points, 1.1 SD below the norm) and Section 3 (16 points, 0.09 SD below the norm) (Table 1), but these results may be explained by serendipitous correct responses to multiple-choice items as the patient stated that they had little understanding of the task. Thus, developmental prosopagnosia was diagnosed based on test results and medical history.
During hospitalization, sleep hygiene instruction, behavioral therapy using the token economy method, group psychotherapy, and rehabilitation were provided, and the patient’s sleep disturbance and functional headache improved sufficiently to permit discharge within three weeks. The token economy method demonstrated efficacy in enhancing the patient’s lifestyle by creating and adhering to a list of desired behaviors, including daytime activities and an ideal bedtime, which were then rewarded with tokens. One month after discharge, however, sleep disturbance and physical symptoms worsened. Based on medical history and results of the DSRS-C (Table 1), we considered these symptoms of depression and initiated treatment. Indeed, sleep disorder, physical symptoms, and depressed mood were all improved by sertraline hydrochloride as the dosage was titrated up to 75 mg/day. Subsequently, the patient enrolled in a private correspondence high school, where communication with friends and teachers was facilitated through an online avatar, and successfully adapted to this mode of interaction.
Table 1: Clinical and Neuropsychological Assessment results of the presented case.
|
Clinical Assessment |
||||||
|
Test |
ADHD RS-IV |
SRS-II |
SDQ |
SCAS |
DSRS-C |
MINI-KIDS |
|
Results |
hyperactivity and impulsivity (7): 1 |
RIRB (60): 62 |
emotional symptoms (4): 6 |
separation anxiety (5): 1 |
score (16): 20 |
dysthymia |
|
(cut off) |
attentional deficit (9): 9 |
SCI (60): 60 |
conduct problems (4): 2 |
social phobia (8): 4 |
|
suicidal risk |
|
|
total score (14): 10 |
total score (60): 61 |
hyperactivity/inattention (6): 3 |
OCD (7): 6 |
|
specific phobia |
|
|
|
|
peer problems (4): 7 |
panic/agoraphobia (7): 3 |
|
N/A except above |
|
|
|
|
prosocial behavior (≤5): 0 |
physical injury fears (7): 3 |
|
|
|
|
|
|
|
generalized anxiety (8): 8 |
|
|
|
|
|
|
|
|
|
|
|
Neuropsychological Assessment |
||||||
|
Test |
WISC-IV |
DN-CAS |
PI-20 |
CFMT |
|
|
|
Results |
Full scale Intelligence Quotient: 111 |
Full Scale: 103 |
81 out of 100 (+2.32SD) |
Section 1: 15 (-6.41 SD) |
|
|
|
|
Verbal Comprehension Index: 88 |
Planning: 96 |
|
Section 2: 19 (-1.1 SD) |
|
|
|
|
Perceptual Reasoning Index: 127 |
Simultaneous: 109 |
|
Section 3: 16 (-0.09 SD) |
|
|
|
|
Working Memory Index: 112 |
Attention: 93 |
|
|
|
|
|
|
Processing Speed Index: 110 |
Successive: 110 |
|
|
|
|
Abbreviations: ADHD RS-IV, ADHD-Rating Scale-IV; CFMT, Cambridge Face Memory Test; DN-CAS, Das-Naglieri Cognitive Assessment System; DSRS-C, Depression Self-Rating Scale for Children; MINI-KIDS, The Mini International Neuropsychiatric Interview for Children and Adolescents; OCD, obsessive compulsive disorder; PI-20, the 20-item Prosopagnosia Index; RIRB restricted interests and repetitive behavior; ROCF, Rey-Osterrieth complex figure test; SCAS, The Spence Children's Anxiety Scale; SCI, social communication and interaction; SDQ, The strengths and difficulties questionnaire; SRS-2, The Social Responsiveness Scale-2; WISC-IV, Wechsler Intelligence Scale for Children IV
Discussion
We present the case of an adolescent female with developmental prosopagnosia who also exhibited symptoms of generalized anxiety disorder and depression, likely due in part to interpersonal problems stemming from the facial recognition deficit. While this is the first reported case to our knowledge, recent studies suggest that developmental prosopagnosia is relatively common but undiagnosed, suggesting that it may be a contributing factor in certain cases of adolescent depression and anxiety.
Statements by the patient and the patient’s mother suggested the presence of prosopagnosia at least since elementary school, although the patient was able to adapt during this period. Developmental prosopagnosia was confirmed by poor performance on the PI-20 (score > 2 SD above the norm) and especially Section 1 of the CFMT (6.41 SD below the norm), although results on CFMT Sections 2 and 3 were closer to the norm for typically developing individuals. Previous studies have reported that CFMT Section 1 scores are substantially higher than normal (indicative of poorer performance) among developmental prosopagnosia patients12 because the items are relatively easy for typically developing individuals. Contrarily, Sections 2 and 3 are challenging even for typically developing individuals, with lower mean scores and larger SD than Section 1. Responses are multiple-choice, and the impact on judgment is more significant in Sections 2 and 3 if the respondent answers without confidence and chooses the correct answer by chance. The results for Sections 2 and 3 were within 2 SD of the norm in this case, but the patient stated that the test was too difficult to understand, so serendipitously correct answers likely influenced the results. Therefore, despite closer-to-normal performance on Sections 2 and 3, the diagnosis of developmental prosopagnosia is still valid considering the totality of the test results and statements by the case patient. The WISC-IV indicated a discrepancy between Verbal Comprehension and the rest of the indexes. Additionally, the attention-deficit/hyperactivity disorder (ADHD) Rating Scale-IV revealed an attentional deficit score above the cutoff. Neurodevelopmental disorders often cluster and co-occur with developmental prosopagnosia, and ADHD is reported as a comorbidity. Hence, the high attentional deficit score may be associated with her ADHD trait; however, we did not diagnose her with ADHD due to her developmental and current history.
In this case and possibly many others, the social effects of developmental prosopagnosia may be partially mitigated in environments providing non-facial clues to identity. After entering junior high school, however, the patient experienced greater difficulty identifying others due to school regulations regarding uniforms and hairstyle. The patient stated that “It was difficult for me to call out my friends’ names and talk to them, and it affected my difficulty going to school,” suggesting deleterious effects on interpersonal relationships. The temporal association between these interpersonal problems and symptom emergence strongly suggests that the onset of generalized anxiety disorder and depression resulted from developmental prosopagnosia.
While there have been a few sporadic reports on the effects of prosopagnosia on interpersonal relationships10, we are aware of no case reports on comorbid psychopathologies, such as depression and anxiety, related to developmental prosopagnosia. A schematic illustrating the clinical course of the case patient according to the Bio–Psycho–Social model is shown in Figure 1. Given this plausible series of events, it is noteworthy that there have been no case reports of anxiety disorders or depression associated with developmental prosopagnosia.
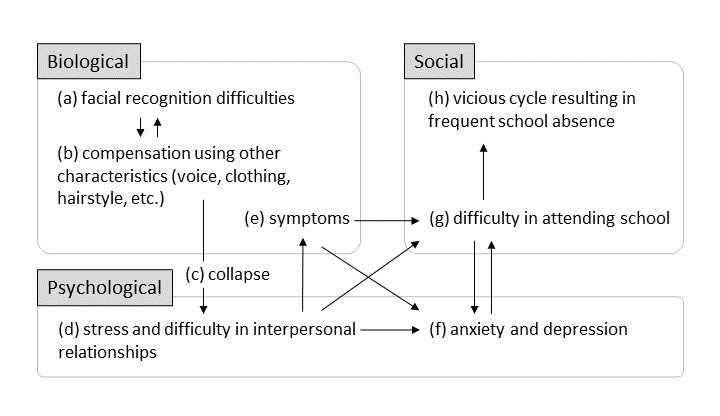
Figure 1: Clinical course of the case patient according to the Bio–Psycho–Social model
Footnote: Schematic of the interactions among biological, social, and psychological factors identified in a female adolescent with developmental prosopagnosia leading to depression and anxiety. (a) The patient experienced facial recognition difficulties even in elementary school, but (b) was able to compensate by relying on other non-facial features such as voice, hairstyle, clothing, and body shape for identification. (c) In junior high school, however, school regulations eliminated these individual identifying features and (d) the stress and difficulty in starting and maintaining interpersonal relationships led to (e) stress-related symptoms such as functional headache and sleep disorder, which (f) exacerbated depression and anxiety, and (g) led to poor attendance. (h) Missing school in turn generated conflict, agitation, and social isolation, which further exacerbated depression and anxiety, forming a vicious cycle.
One possible reason is that developmental prosopagnosia is not well recognized10. Although prosopagnosia is listed as agnosia in ICD11, it is not listed in the DSM54 and there are no standard diagnostic criteria. Therefore, even if patients are aware of facial recognition difficulties, it is unlikely that many will receive medical attention. In addition, patients with developmental prosopagnosia have likely used compensatory mechanisms to identify others since childhood and so may be unaware of their facial recognition difficulties or consider them insignificant1.
In addition, situations that preclude non-facial recognition may be less common in countries where there are fewer strict regulations on dress or appearance*. Furthermore, people with developmental prosopagnosia may have less difficulty in multiethnic countries where individuals can be identified by combinations of prominent features not shared by others in the group. Therefore, even if developmental prosopagnosia is recognized, compensation is relatively easy. Conversely, interpersonal problems may be more common in ethnically homogeneous countries with stricter guidelines on appearances such as Japan. To prevent interpersonal problems and secondary psychiatric disorders related to prosopagnosia, it may be helpful to conduct early screening and intervention before adolescence when sociality is developing and friendships are becoming more complex. Further research is needed in this topic in the future.
Considering an alternative perspective, although there are reports linking prosopagnosia to anxiety and depression, the causal relationship remains controversial8,9. Additionally, there are reports of impaired face recognition in depressed patients13, complicating the determination of a causal relationship between prosopagnosia and depression. To elucidate this relationship, a thorough examination of the medical history is essential.
Nonetheless, it is possible that there are many undiagnosed cases of developmental prosopagnosia even in Western countries9 that may increase the risks of anxiety and depression. Early detection is of utmost importance to provide appropriate intervention. For this purpose, it is essential to consider the possibility of developmental prosopagnosia when treating patients with difficulties in interpersonal relationships and social functioning. Particular attention should be paid to the possibility that compensatory strategies may be ineffective in certain environments, such as when the patient needs to interact with many new people after entering higher education, changing schools, or finding a new job.
References
- Duchaine BC, Nakayama K. Developmental prosopagnosia: A window to content-specific face processing. Curr Opin Neurobiol. 2006; 16(2): 166-173.
- Bodamer J. Prosop’s agnosia; the agnosia of cognition. Arch Psychiatr Nervenkr Z Gesamte Neurol Psychiatr. 1947; 118(1-2): 6-53.
- McConachie HR. Developmental prosopagnosia. A single case report. Cortex. 1976; 12(1): 76-82.
- American Psychiatric Association. American Psychiatric Association. DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
- Bowles DC, McKone E, Dawel A, et al. Diagnosing prosopagnosia: Effects of ageing, sex, and participant–stimulus ethnic match on the Cambridge Face Memory Test and Cambridge Face Perception Test. Cogn Neuropsychol. 2009; 26(5): 423-455.
- Behrmann M, Avidan G, Gao F, et al. Structural imaging reveals anatomical alterations in inferotemporal cortex in congenital prosopagnosia. Cereb Cortex. 2007; 17(10): 2354-2363.
- Yardley L, McDermott L, Pisarski S, et al. Psychosocial consequences of developmental prosopagnosia: A problem of recognition. J Psychosom Res. 2008; 65(5): 445-451.
- Davis JM, McKone E, Dennett H, et al. Individual differences in the ability to recognise facial identity are associated with social anxiety. PLoS One. 2011; 6(12): e28800.
- Pressl C, Jiang CS, Correa da Rosa J, et al. Interrogating an ICD-coded electronic health records database to characterize the epidemiology of prosopagnosia. J Clin Transl Sci. 2020; 5(1): e11.
- Shah P, Gaule A, Sowden S, et al. The 20-item prosopagnosia index (PI20): A self-report instrument for identifying developmental prosopagnosia. R Soc Open Sci. 2015; 2(6): 140343.
- Nakashima SF, Ukezono M, Sudo R, et al. Development of a Japanese version of the 20-item prosopagnosia index (PI20-J) and examination of its reliability and validity. JJ Pshicho. 2020; 90(6): 603-613.
- Duchaine B, Nakayama K. The Cambridge Face Memory Test: Results for neurologically intact individuals and an investigation of its validity using inverted face stimuli and prosopagnosic participants. Neuropsychologia. 2006; 44(4): 576-585.
- Guyer AE, Choate VR, Grimm KJ, et al. Emerging depression is associated with face memory deficits in adolescent girls. J Am Acad Child Adolesc Psychiatry. 2011; 50(2): 180-190.