
The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers
Simon Xin Min Dong*
International Institute of Consciousness Science®, Vancouver, BC, Canada
Abstract
Peptic ulcers, including duodenal and gastric ulcers, are currently studied as an infectious disease caused by Helicobacter pylori. However, this etiology cannot elucidate the major characteristics and observations/phenomena of the disease, as well as the roles of gastric acid and NSAIDs. Additionally, many patients with severe ulcer symptoms have no infection, suggesting bacterial eradication cannot prevent relapses in all ulcer patients. To address these challenges, a recently published Complex Causal Relationship with its accompanying methodologies was applied to analyze the existing data. Peptic ulcers were identified as a psychosomatic disease triggered by psychological stress, where Helicobacter pylori plays a secondary role in only the late phase of ulceration. An integration of five major etiological theories in history illustrated the entire pathogenesis of peptic ulcers, which addressed all the characteristics, observations/phenomena, controversies, and mysteries of the disease in a series of 6 articles. This first article focuses on the pathogenesis of duodenal ulcers. The hyperplasia and hypertrophy of gastrin and parietal cells induced by chronic stress potentiate the individual’s response to immediate stress, resulting in the hypersecretion of gastric acid and eventually, duodenal ulceration. This psychopathological mechanism resolved all the controversies associated with Helicobacter pylori and explicitly elucidated 7 characteristics of duodenal ulcers, as well as 42 observations/phenomena. The roles of gastric acid, Helicobacter pylori, and NSAIDs in duodenal ulcers were also identified. The effectiveness validated the etiology of duodenal ulcers identified by the Complex Causal Relationship, indicating stress management is essential for a complete cure of the disease without relapse.
Introduction
Peptic ulcer disease, including duodenal and gastric ulcers, is a serious medical condition in the upper gastrointestinal tract, affecting ~10% of the world population1. Over the centuries, 13 etiological theories, such as ‘No Acid, No Ulcer’ (1910)2, Nerve Theory (1913)3, Psychosomatic Theory (1950)4, and Stress Theory (1950)5, have been proposed to explain its pathogenesis6. Although each of these theories could explain some characteristics and observations/ phenomena of peptic ulcers, they failed to explain the majority of these due to their respectively challenging inconsistencies7.
In 1987, Marshall proposed that peptic ulcers are an infectious disease caused by the infection of Helicobacter pylori (H. pylori)8. This etiological theory has been designated as Theory of H. pylori6. However, this theory is not superior to any other theory in history, but has led to additional controversies and challenges in the field9–13. It cannot explain most of the 15 characteristics and 81 observations/ phenomena of peptic ulcers6, including 30 of the 36 observations/phenomena associated with the bacterium itself. For example, provided H. pylori is the cause of peptic ulcers, all patients should have the infection, but ulcers in 20~40% patients are idiopathic14,15, indicating not all patients are infected. Interestingly, many patients with severe ulcer symptoms have no infection13,16, suggesting that bacterial eradication cannot prevent the relapse in these patients17. Moreover, how the infection leads to ulceration remains unknown and the roles of gastric acid and Non-steroidal Anti-inflammatory Drugs (NSAIDs) in the disease have never been elucidated15,18, thus exemplifying the pitfalls of this theory. Furthermore, this etiology cannot elucidate the birth-cohort phenomenon, seasonal variation, and African enigma of peptic ulcers, as well as the morphology and predilection sites of gastric ulcer.
The progress on all other diseases is similar to peptic ulcers. To date, no disease has been fully understood. To address these challenges, I investigated the successful, historical, scientific research in fields outside the scope of medical science and found inspirations from the realm of physics. Newton established the first causal relationship in 1687 in his Law of Universal Gravitation, and Einstein established the second causal relationship in 1905 in his Mass-energy Equation. The two historic universal causal relationships allowed major progress to be made in macro- and micro-physics, respectively. The successes in physics suggest that establishing a universal causal relationship for life science and medicine may be essential to understand life phenomena and human diseases.
In May 2012, a new causal relationship, the Complex Causal Relationship (CCR), was proposed for life science and medicine19. The CCR can be explained by drawing a parallel to Newton’s Law of Universal Gravitation or Einstein’s Mass-energy Equation. In both historic causal relationships, Newton and Einstein considered two essences of their research subjects: the visible, tangible, and corporeal MASS, which was defined as the Concrete Essence; and the invisible, intangible, and incorporeal Force or Energy, which was defined as the Abstract Essence. In physics, the apple falls to the ground due to its Abstract Essence, Force, and electrons transition to new orbitals due to absorption or release of the Abstract Essence, Energy. The CCR dictates that, similar to the research subjects in physics, the human body also has both Concrete Essence and Abstract Essence, and the human body suffers from various diseases due to its Abstract Essence19. However, the Abstract Essence of the human body has rarely been investigated in modern medicine.
I hypothesize that taking the Abstract Essence of the human body into consideration may allow us gain unprecedented insights into any disease. To test this hypothesis, peptic ulcers were selected as a model disease, and the CCR with its accompanying methodologies was applied to analyze the existing data. Encouragingly, the data analyses can address all the controversies, mysteries, characteristics, and observations/phenomena of peptic ulcers. Due to a limit of words, the data analyses were summarized into a series of 6 articles (Supplementary Table S1). This article is the first one, focusing on the pathogenesis of duodenal ulcers. Notably, numerous historical studies, especially those from 1900 to 1990, are extremely valuable for a full understanding of the pathogenesis of peptic ulcers.
Methods
Four steps were taken to analyze the existing data. First, the CCR served as a benchmark to pinpoint the etiology of peptic ulcers from the 13 theories in history. Second, the application of a novel methodological concept, Integral Perspective19, integrated 5 major etiological theories into one single theory. Third, another novel methodological concept, Superposition Mechanism19, was employed to explain the clinical, epidemiological, and laboratory observations of duodenal ulcers. Lastly, the roles of gastric acid, H. pylori, and NSAIDs in duodenal ulcers were elucidated.
Results
A definite etiology with effective analytical methods is required for a full understanding of disease. Herein the application of the CCR with its accompanying methodologies helped to achieve this goal. Fortunately, modern medicine has accumulated enough empirical data for data analyses.
The application of the CCR identified the etiology of peptic ulcers
The CCR dictates that although the Abstract Essence of the human body is invisible, intangible, and incorporeal, it is the driving force of life phenomena and human diseases, indicating that the early phase of any disease is an abstract process. Based on this concept, out of all the 13 etiological theories6, only Psychosomatic Theory and Stress Theory suggested invisible, intangible, and incorporeal causes for peptic ulcers as shown in Table 1. Both theories were supported by numerous data from clinical and epidemiological observations5,20–22, and were demonstrated reproducible23–30. Psychosomatic Theory focuses more on the impact of mental health related to past life experiences, whereas Stress Theory concentrates on the influence of current life events. When combining the two theories, I elucidate that psychosomatic factor makes the individual susceptible to current psychological stress, leading to peptic ulcers. Concisely, a combination of the two etiological theories suggests that peptic ulcers are a psychosomatic disease triggered by psychological stress.
Ford and Talley insisted that there is a causal relationship between H. pylori and duodenal ulcers9, whereas Hobsley believed that gastric acid plays a more important role than H. pylori in the disease10. Currently, NSAIDs are also considered a cause of peptic ulcers15,31. However, H. pylori, gastric acid, and NSAIDs are not invisible, intangible, and incorporeal and thus, none of the 3 concrete factors match the standard set by the CCR to be the cause of disease. This explains why the etiologies based on H. pylori, gastric acid, or NSAIDs cannot explain the pathogenesis of peptic ulcers, despite supports from clinical or epidemiological observations. In fact, the hypersecretion of gastric acid may not be a cause but an effect of psychological stress, as observed in clinical patients32,33. Additionally, there are 30- 40% idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients34, also suggesting that neither H. pylori nor NSAIDs is the cause of peptic ulcers.
Integrating five major etiological theories in history into one single theory
Next, the 13 etiological theories in history were further examined6. Five of them have been studied in more details and were supported by numerous clinical, epidemiological, and laboratory data (Table 1). Interestingly, each of the five major theories focused on only one area of the human body. For example, Nerve Theory only focused on abnormal neurotransmitters in the brain, ‘No Acid, No Ulcer’ was solely concerned with the hypersecretion of gastric acid, and Theory of H. pylori concentrated exclusively on bacterial infection in the upper digestive tract.
Table 1: Summary of Selected Studies
|
Etiological Theories |
Founder & Year |
Repeat Example |
Key Points |
|
1. No Acid, No Ulcer2 |
Dragutin (Carl) Schwartz, 1910 |
P. Miner, 200435 |
The hypersecretion of gastric acid is the cause of peptic ulcers. |
|
2. Nerve Theory3 |
Von Bergmann G., 1913 |
G.B. Glavin, et al.,199136 |
The abnormality of neurotransmitters in the central nervous system is the cause of peptic ulcers. |
|
3. Psychosomatics Theory4 |
Franz Gabriel Alexander, 1950 |
Mark Feldman, et al., 198623 |
Social, psychological, and behavioral factors are the cause of peptic ulcers. |
|
4. Stress Theory5 |
Hans Selye, 1950 |
Michael P. Jones, 200637 |
Stress induced by personality traits, and social and natural events is the cause of peptic ulcers. |
|
5. Theory of H. Pylori8 |
Barry J. Marshal and J. Robin Warren, 1987 |
Furuta, et al., 199838 |
Peptic ulcers are an infectious disease caused by the infection of H. pylori. |
a. Dong, S. X. M., Chang, C. C. Y. & Rowe, K. J. A collection of the etiological theories, characteristics, and observations/phenomena of peptic ulcers in existing data. Data Br. 19, 1058–1067 (2018).
b. The etiological theory based on the infection of H. pylori was designated as Theory of H. pylori.
Newton’s Law of Universal Gravitation suggests that due to the abstract essence of the apple and the earth, Force, the two objects are not independent entities but an ‘inseparable integrity’. Similarly, the CCR suggests that, due to the abstract essence of the human body, all the individual organs are not independent pieces, but an ‘inseparable integrity’. This concept is termed ‘integral perspective’19, which indicates that integrating the five major theories on peptic ulcers into one single theory may gain unprecedented insights into the disease. Excitingly, an integration of the five major theories, Psychosomatic Theory, Stress Theory, Nerve Theory, ‘No Acid, No Ulcer’, and Theory of H. pylori (Table 1) did paint a complete picture of the pathogenesis of peptic ulcers, including the early, intermediate, and late phases of peptic ulcerations. Psychosomatic Theory and Stress Theory illustrate the early phase of peptic ulcers, in which abstract psychosomatic factors and psychological stress initiate the disease. Nerve Theory bridges the gap between the early and the late phases of peptic ulcerations, uncovering the consequences of psychological stress that aberrant nerve impulses are transmitted to the stomach36, resulting in the hypersecretion of gastric acid in duodenal ulcer, or the pathological lesions in gastric ulcer. The late phase of peptic ulceration is a corrosive process caused by local aggressive factors in the stomach as described in ‘No Acid, No Ulcer’ and Theory of H. pylori. For ease of narration, the new theory originated from the integration is termed Theory of Nodes. More details on how this term is derived will be given in the second article of the series on the pathogenesis of gastric ulcer.
The Pathogenesis of Duodenal Ulcer
Theory of Nodes divides the entire process of duodenal ulceration into early, intermediate, and late phases. The mechanism of gastric acid hypersecretion is the key pathological process to elucidate all the clinical, epidemiological, and laboratory observations/phenomena of duodenal ulcers, as well as the roles of gastric acid, H. pylori, and NSAIDs in the disease. Notably, each of the three phases described herein is supported by a large amount of existing data.
Early phase: the hyperplasia and hypertrophy of gastrin and parietal cells
In Theory of Nodes, hereditary predisposition determines that psychosomatic factors, such as hypochondriasis, a negative perception of life events, dependency, and lowered self-confidence23, make a portion of individuals in the population more susceptible to environmental factors than others. Existing data discovered a positive correlation between stressful occupations and duodenal ulcers21,39, and duodenal ulcers were associated with bad habits, poor lifestyle, laborious work, unhealthy environment, and long-term emotional distress40. These findings suggest that the early phase of duodenal ulcer is a long-term/ chronic pathophysiological process41. Life in large cities is more competitive and stressful than in rural areas42,43, explained the higher incidence of duodenal ulcers in large cities44. Psychosomatic factors or chronic stressors constantly provoke the neurotransmitter release in the central nervous system and thus, duodenal ulcers are a ‘brain-driven event’36 often accompanied by psychological disturbances such as anxiety, neuroticism, depression, somatization, or poor appetite27,45.
Constant and prolonged releases of neurotransmitters in the central nervous system lead to an extremely complex pathophysiological process, in which distinct neural networks regulate the functions of multiple peripheral organs36, resulting in the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach46,47. Existing data suggests that at least four pathways are involved in this chronic process (Figure 1): 1. Bad habits in eating, drinking, and smoking48–50 or long-term drug usage51 cause ‘local’ chronic stress in the stomach. For example, drinking a large volume of water immediately after lunch significantly lowers the concentration of gastric acid. The increased pH is constantly sensed and regulated by the enteric nervous system, causing increased parietal cell mass and hyperplasia of gastrin cells52,53 (Figure 1a). 2. Vagus nerves play a key role in gastric secretion; tensions, emotional strains, and competitive efforts of modern life result in hypertonus in the vagus nerves54. The hyperplasia of gastrin cells was observed after bilateral truncal vagotomy55, indicating brain-gut axis may induce the hyperplasia of gastrin cells due to vagus nerve dysfunction (Figure 1b). 3. Prolonged exposure to stress activates the hypothalamus-pituitary-adrenal (HPA) axis, causing the hyperplasia and hypertrophy of adrenaline56,57 and the subsequent high level of hormones from adrenaline may induce the hyperplasia and hypertrophy of gastrin and parietal cells58 (Figure 1c). 4. Chronic stress may induce hyperplasia and hypertrophy of parathyroid glands, which were also reported to be associated with duodenal ulcer59,60 (Figure 1d).
In Theory of Nodes, the pathways to induce the hyperplasia and hypertrophy of gastrin and parietal cells vary individually due to heredity and past life experiences, and the degrees of hyperplasia and hypertrophy to induce duodenal ulcers range from mild, moderate, to severe, which is associated with the local aggressive factors in the gastroduodenum, especially the infection of H. pylori. In addition, a birth-cohort study found ‘the trends for duodenal ulcers were similar to gastric ulcers but followed ~5 years behind’61, indicating it usually takes ~5 years to induce the hyperplasia and hypertrophy. This chronic pathophysiological process is hard to duplicate in the lab, making it difficult to establish animal models for stress- induced duodenal ulcers36.
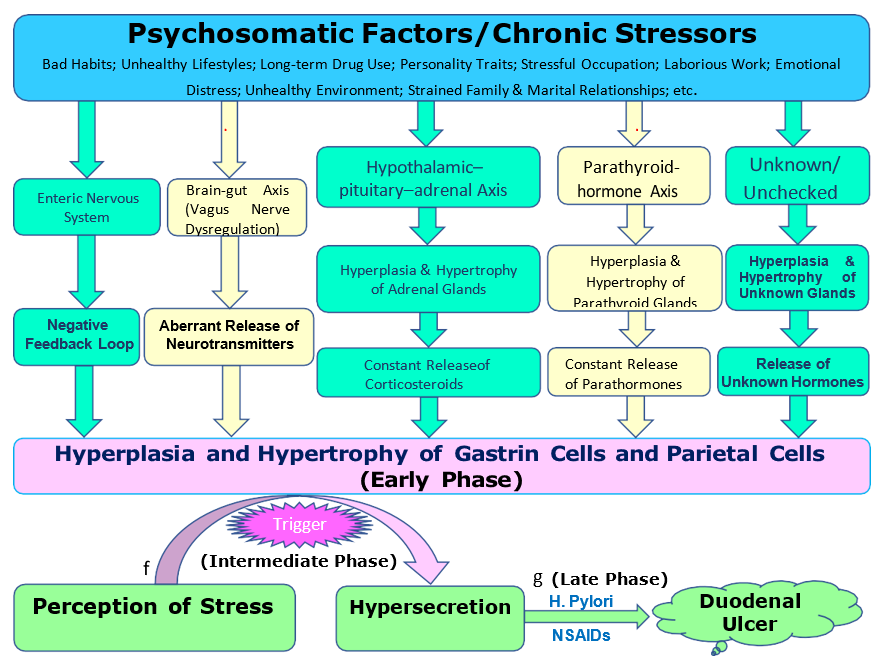
Figure 1: Chronic stress induces hyperplasia and hypertrophy of gastrin and parietal cells.
Multiple pathways are involved in the hyperplasia and hypertrophy of gastrin and parietal cells. (a) Local stress in the stomach induced by bad habits or long-term drug use is sensed and regulated by the enteric nervous system, causing hyperplasia and hypertrophy of gastrin and parietal cells via a negative feedback loop. (b) Chronic stress leads to vagus nerve dysfunction via the brain-gut axis, resulting in the hyperplasia of gastrin cells. (c) Prolonged exposure to stress activates the HPA axis, inducing the hyperplasia and hypertrophy of adrenaline. The subsequent high level of corticosteroids causes hyperplasia and hypertrophy of gastrin and parietal cells. (d) Chronic stress induces the hyperplasia and hypertrophy of gastrin and parietal cells via the parathyroid-hormone axis. (e) There might be other unknown or unchecked pathways. Pathways a, b, c, d, and e lead to the hyperplasia and hypertrophy of gastrin and parietal cells in the early phase. (f) Due to the hyperplasia and hypertrophy of gastrin and parietal cells, the perception of stress triggers the hypersecretion of gastric acid in the intermediate phase. (g) The hypersecretion of gastric acid, long with H. pylori, NSAIDs, and other local aggressive factors, results in duodenal ulcerations in the late phase.
Intermediate phase: hypersecretion of gastric acid triggered by stress
Compared to the long-term early phase, the intermediate phase is a short-term process characterized by stress-triggered hypersecretion of gastric acid (Figure 1f). A case-control study discovered that traumatic life events commonly preceded the onset of peptic ulcers62. Another study found that acute events or chronic stressors were substantially associated with the onset and relapse of duodenal ulcers41. Symptomatic exacerbations of peptic ulcers occurred during or shortly after stressful events29,33. These studies suggest that duodenal ulcer is a disease triggered by the perception of stress. On the other hand, many studies demonstrated that duodenal ulcer patients had higher basal and maximal gastric acid secretion35,63. Thus, ‘No Acid, No Ulcer’ is a true statement for duodenal ulcers. In Theory of Nodes, the hypersecretion of gastric acid is triggered by the perception of stress via vagus nerves, and the hyperplasia and hypertrophy of gastrin and parietal cells induced in the early phase potentiate the individual’s response to life events. As a result, even trivialities may trigger the hypersecretion of gastric acid, leading to duodenal ulcers.
However, the sources of stress are not limited to life events. A multivariate analysis found that two chronic stressors, personal threat and goal frustration, were also associated with the onset and relapse of duodenal ulcers41, indicating the perception of stress might be spontaneous without the experience of a life event. Ulcer patients with many other stressors unrelated to life events, such as chronic marital distress and conflict or dislike of living/working environments, may not be investigated in epidemiological surveys such as in questionnaires, but were included in the control group, resulting in conclusions like ‘there is no definitive study proving a causal relationship between psychological stress and the development of ulcer disease37,64. It is not surprising that, of all 33 patients with active ulcers, only 16 symptomatic patients had been preceded by severe stress and more pathological results from the Minnesota Multiphasic Personality Inventory29. These suggest that questionnaire-based epidemiological surveys40,64 may have discounted many chronic stressors, and the methodologies essential to study psychosocial factors (the abstract essence of the human body) have yet to be established.
Late phase: symptomatic ulcer
Compared to the long-term early phase, the intermediate phase is a short-term process characterized by stress-triggered hypersecretion of gastric acid (Figure 1f). A case-control study discovered that traumatic life events commonly preceded the onset of peptic ulcers62. Another study found that acute events or chronic stressors were substantially associated with the onset and relapse of duodenal ulcers41. Symptomatic exacerbations of peptic ulcers occurred during or shortly after stressful events29,33. These studies suggest that duodenal ulcer is a disease triggered by the perception of stress. On the other hand, many studies demonstrated that duodenal ulcer patients had higher basal and maximal gastric acid secretion35,63. Thus, ‘No Acid, No Ulcer’ is a true statement for duodenal ulcers. In Theory of Nodes, the hypersecretion of gastric acid is triggered by the perception of stress via vagus nerves, and the hyperplasia and hypertrophy of gastrin and parietal cells induced in the early phase potentiate the individual’s response to life events. As a result, even trivialities may trigger the hypersecretion of gastric acid, leading to duodenal ulcers.
For individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcers. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcer may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients14. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid, can induce acute and chronic duodenal ulcer in normal rats66, whereas inoculation of H. pylori alone cannot11,67, further indicating that gastric acid plays a more important role than H. pylori in duodenal ulcers. Gastric acid, H. pylori, and NSAIDs play a role in only the late phase of ulceration, suggesting duodenal ulcer is not initiated by any of the 3 local aggressive factors. Unequivocally, none of them is an etiological factor of the disease.
The Superposition of Local Aggressive Factors in The Gastro-Duodenum
Most of the controversies on peptic ulcers concentrate on the late phase of ulceration, especially on the roles of H. pylori, gastric acid and NSAIDs. To further understand the late phase of duodenal ulceration, herein the existing data on all known local aggressive factors in the stomach was analyzed. Interestingly, the local aggressive factors were studied as separate entities in modern medicine, and they have never been considered a combinatorial force to corrupt the mucosa. The concept of integral perspective dictates that a pathological process is usually caused not by an individual aggressive factor, but by multiple factors based on Superposition Mechanism, which takes into account that factors with commonalities can have additive effects19. Existing data indicates that the hypersecretion of gastric acid is a determinant factor in the late phase of duodenal ulceration10,68, but all the other local aggressive factors also contribute to the corrosive intensity69, ultimately resulting in duodenal ulceration when the total corrosive intensity exceeds the resistance of duodenal mucosa. Therefore, it is the total sum of corrosive intensities from all local aggressive factors acting on duodenal bulb that leads to the characteristic erosive appearance of duodenal ulcers. To illustrate the Superposition Mechanism, herein 21 hypothetical cases with different local aggressive factors that may lead to ulceration were generated in Figure 2. These hypothetical cases are a summary of data from epidemiological and clinical studies.
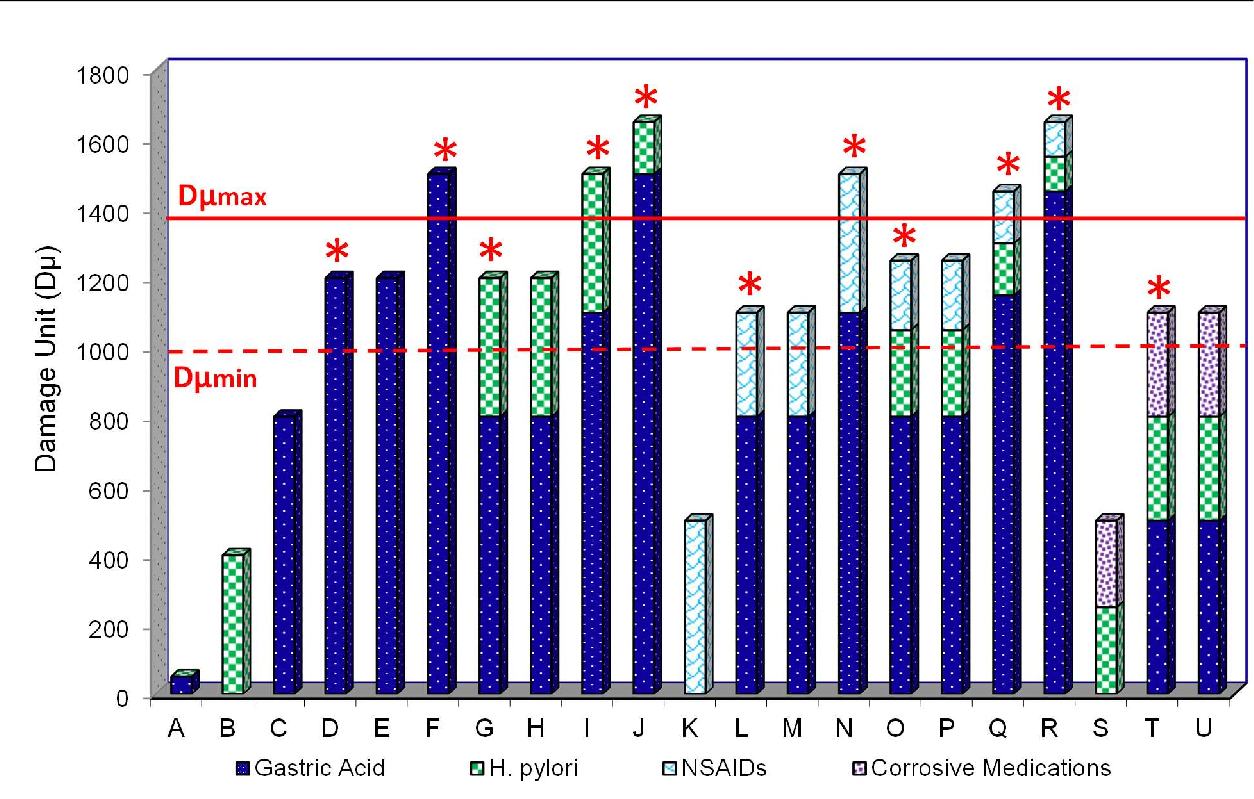
Figure 2: The superposition mechanism of local aggressive factors in duodenal ulceration.
The data in the graph is representative of different hypothetical situations where local aggressive factors create an additive effect that may lead to ulceration. The hypersecretion of gastric acid is a determinant factor in duodenal ulceration, but all the other local aggressive factors are also involved. The corrosive intensity caused by an aggressive factor was defined as Damage Unit (Dμ), and the total sum of corrosive intensities of each case (ΣDµ) is calculated individually by the formula: ΣDµ = DμGastric Acid+DμH. pylori+DμNSAIDs+DμCorrosive Medications. Due to distinct genetic backgrounds and life experiences, the susceptibility of duodenal mucosa varies individually. Accordingly, each individual has her/his own threshold of ulceration. Therefore, a theoretical range between Dμmin and Dμmax was set as the threshold of ulceration. ΣDμ values per individual case below Dμmin (dash line) will not result in ulceration, ΣDμ values above Dμmax (solid line) will result in ulceration, and ΣDμ values within the range may or may not result in ulceration. When the ΣDμ value falls between Dμmin and Dμmax, even though some individuals have the same ΣDμ value, the one whose duodenal mucosa is more susceptible to the local aggressive factors are more likely to ulcerate. *Indicates cases of ulceration.
In Figure 2, Case A demonstrates an H. pylori-negative healthy individual who has normo-secretion and suffers no damage (Dμ=0). This is the baseline for normal, healthy individuals. Case B represents the most common situation for individuals with normo-secretion and H. pylori infection. Although they suffer damage from the H. pylori infection, the ΣDμ value does not reach the lowest threshold, Dμmin, meaning the individuals do not suffer from ulceration. Cases C, D, E and F are H. pylori-negative examples where different degrees of hypersecretion determine the ΣDμ value. value. Case C does not ulcerate (ΣDμC<Dμmin), Case D ulcerates because Dμmin<ΣDμD<Dμmax and Case F has high- range hypersecretion (ΣDμF>Dμmax), which results in ulceration. Although Case E has the same ΣDμ as Case D (ΣDμE=ΣDμD), Case E does not ulcerate because her/his duodenal bulb mucosa is less susceptible than Case D.
Cases G and H give examples of patients with similar ΣDμ values due to corrosive intensity from superposition of both low-range hypersecretion of gastric acid and H. pylori infection. Both cases are within the range for potential ulceration, however, the individuals in Cases G and H have different mucosal susceptibility; therefore, Case G progresses to ulceration whereas Case H does not. Case I represents the ΣDμ value for hypothetical H. pylori-positive patients with mid-range hypersecretion. Although the corrosive intensity of acid alone does not overcome the individual’s mucosal resistance to ulceration, with the addition of the damage from H. pylori the ΣDμ value surpasses Dμmax and therefore, the patient suffers ulceration. Case J is an example of H. pylori-positive patients with high-range hypersecretion. With or without the damage from H. pylori, the hypersecretion exceeds Dμmax, resulting in ulceration. Case K illustrates normo-secretion with NSAIDs use, wherein the ΣDμ value does not reach Dμmin. The damage from the NSAIDs alone is not enough to cause ulceration. Cases L and M represent the additive damage of low-range hypersecretion and NSAIDs usage. In both cases, the damage from the gastric acid alone does not reach Dμmin, but with the addition of the corrosive intensity from NSAIDs, the ΣDμ enters the threshold for potential ulceration. However, only Case L ulcerates because her/his duodenal mucosa is more susceptible to local aggressive factors than Case M. Case N is an example of the additive damage of mid-range hypersecretion and NSAIDs usage, but in this case, the patient ulcerates because DμGastric Acid + DμNSAIDs>Dμmax.
Cases O and P illustrate H. pylori-positive individuals with low-range hypersecretion and NSAIDs usage, wherein Dμmin<ΣDμ<Dμmax. However, only Case O ulcerates because this individual is more susceptible than Case P. Case Q represents the ΣDμ value for H. pylori-positive, NSAIDs using patients with mid-range hypersecretion. Although the corrosive intensity of the hypersecretion of gastric acid alone is less than Dμmax, the addition of the damage from H. pylori and NSAIDs causes the ΣDμ value to surpass Dμmax and the patient suffers ulceration. Notably, H. pylori may upregulate the expression of COX-2 and subsequently results in the biosynthesis of gastroprotective prostaglandin, which in turn offsets the corrosive intensity of NSAIDs and thus is conducive to the healing of NSAIDs-induced ulcers70,71, causing ‘H. pylori infection reduces the development of ulcers in NSAIDs users’44. Case R represents the ΣDμ value from high-range hypersecretion, H. pylori infection, and NSAIDs usage wherein the corrosive intensity of the acid alone surpasses Dμmax and causes ulceration. In this case, the Dμ values from H. pylori and NSAIDs do not significantly contribute to the ulceration process. Case S illustrates normo-secretion with H. pylori infection and NSAIDs use, wherein the ΣDμ value does not reach Dμmin. The damage from H. pylori and NSAIDs is not enough to cause ulceration. Cases T and U show similar situations with very low-range hypersecretion, H. pylori infection, and corrosive medications. In these cases, corrosive medication usage, such as chemotherapy drugs, exerts damage on the duodenal bulb causing the ΣDμ value to enter the ulceration threshold. Case T ulcerates, but Case U does not due to different susceptibility.
In summary, cases A, B, C, K, and S have ΣDμ values that are less than Dμmin and do not ulcerate. Cases F, I, J, N, Q, and R are duodenal ulcer patients because their ΣDμ values surpass Dμmax. Cases D, G, L, O, and T have ΣDμ values within the threshold range for ulceration and they ulcerate due to their susceptibility to local aggressive factors. Cases E, H, M, P, and U also have ΣDμ values within the threshold range for ulceration, but they do not ulcerate because the corrosive intensity cannot overcome their individual resistance to local aggressive factors. Cases C, G, H, L, M, O, P, T, and U have mild degree of hyperplasia and hypertrophy of gastrin and parietal cells, Cases D, E, I, N, and Q, have moderate degree of hyperplasia and hypertrophy, and Cases F, J, and R have severe hyperplasia and hypertrophy, which account for the different levels of gastric acid hypersecretion in these cases.
The roles of gastric acid, H. pylori, and NSAIDs in duodenal ulcerations
Figure 2 can elucidate all the observations/phenomena related to gastric acid, H. pylori, NSAIDs and other medications in duodenal ulcers. Since each of the 3 local aggressive factors partially contributes to the corrosive intensity and duodenal ulceration is caused by the total corrosive intensity, the higher density of H. pylori, the higher total corrosive intensity. As a result, H. pylori infection exacerbates clinical symptoms and increases the clinical morbidity/mortality rates of the disease, and so does the NSAIDs usage. In contrast, the eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity/mortality and the rates of re-bleeding in ulcer patients. Cases B to J explain why H. pylori density is associated with the morbidity rate of duodenal ulcers44 and Cases K to R explain that duodenal ulcers in H. pylori-negative patients are presumably due to NSAIDs72. Without the hypersecretion of gastric acid, the corrosive intensity caused by either H. pylori or NSAIDs could not reach the threshold of ulceration. Therefore, H. pylori-positive patients and NSAIDs users require the hypersecretion of gastric acid to progress to duodenal ulcers68, indicating H. pylori infection is not ‘important etiological factor of duodenal ulcers’73, but second to the hypersecretion of gastric acid. For individuals with mild or moderate hyperplasia and hypertrophy of gastrin and parietal cells, H. pylori infection and/or NSAIDs usage significantly increase the corrosive intensities. As a result, although the hypersecretions of gastric acid in those individuals are not enough to induce duodenal ulcers independently, they still suffer from duodenal ulcers because the total sum of corrosive intensities reaches the threshold of ulceration. All these analyses suggest that neither H. pylori infection nor NSAIDs usage is essential for ulceration and they both are not the cause of duodenal ulcers. They play a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA74,75, cannot explain the higher prevalence of duodenal ulcers.
Case B is applicable to most H. pylori-infected individuals, but only those also impacted by the hyper- secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. This explains ‘in spite of a high prevalence of H. pylori infection worldwide, the incidence of duodenal ulcer disease is low’76. The variation of ulcer prevalence is due to different social environments, as shown in the birth-cohort phenomenon61. Comparing Cases C and G demonstrates that the morbidity of duodenal ulcers is increased in H. pylori-infected individuals77. Contrasting Cases D and G or F and I illustrates the conclusion from a study in Northern Italy and Denmark that ‘H. pylori-negative duodenal ulcers were associated with a poorer prognosis mainly because of a higher rate of ulcer and symptom relapse78. To reach the ulceration threshold without the corrosive intensity from H. pylori, the hypersecretion of gastric acid needs to be higher in H. pylori-negative patients. The higher hypersecretion in Cases D and F indicates more severe negative impacts from psychosocial stress than in Cases G and I. Additionally, the damage from H. pylori can be relieved by antibiotics, as in Cases G and I, decreasing the corrosive intensity in these patients, whereas Cases D and F cannot achieve the same therapeutic effect. Therefore, there is a poorer prognosis and a higher relapse rate in H. pylori-negative patients78. Cases D and F were caused simply by the hypersecretion of gastric acid due to psychological stress, which explain 20~40% of patients with idiopathic ulcers14,15 and the eradication of H. pylori cannot prevent the relapse of these cases.
Bleeding suggests that the patients are more likely to have severe hyperplasia and hypertrophy of parietal and gastrin cells and they are seriously impacted by stress as illustrated by Cases F. In that case, H. pylori infection is not essential to reach the threshold for ulceration. In contrast, non-bleeding ulcer suggests the patients are more likely to be slightly impacted by stress with mild hyperplasia and hypertrophy as Case G, and H. pylori infection is essential to reach the threshold for ulceration. As a result, bleeding ulcer patients are more likely to be H. pylori negative and non-bleeding patients are more likely to be H. pylori positive, causing ‘the prevalence of H. pylori in patients with bleeding ulcers may be 15~20% lower than in patients with non-bleeding ulcer’79. Clinical patients suffer the relapses of ulcers80 because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and the hyperplasia and hypertrophy of parietal and gastrin cells, as well as the impact of stress, have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’81,82. Moreover, Figure 2 indicates that the classification of duodenal ulcers into three categories, H. pylori-related, NSAIDs-related, and non-H. pylori/non-NSAIDs-related83, overlooked the determinant factor in duodenal ulceration, the hypersecretion of gastric acid.
Figure 2 further suggests that gastric acid is the primary local aggressive factor in the late phase of duodenal ulcers68 and H. pylori is a secondary contributor to this process, as indicated by Cases D, F, L, and N where ulceration occurs without H. pylori. These four cases support the finding that in some countries, 30-40% of duodenal ulcer patients were H. pylori-negative13 and explain a clinical observation ‘up to 35% of 387 infected patients failed to respond to standard anti-H. pylori therapy’84. Other clinical trials also found that the most common therapies, including proton pump inhibitors plus two antibiotics, were unsuccessful in more than 20% of patients, and in a routine clinical setting, the unsuccessful treatment rate was even greater85. In addition, together with Cases J and R, these cases exemplify that etiological factors other than H. pylori play a significant role in duodenal ulcers because there is a 20% relapse rate within six months despite successful eradication of H. pylori86. Cases J and R also explain that many duodenal ulcers are falsely attributed to H. pylori infection because the majority of the damage in these cases comes from the hypersecretion of gastric acid87. Furthermore, the eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, which are representative of most clinical patients. However, the eradication of H. pylori would not prevent the relapse in H. pylori-negative Cases D and F, or in H. pylori-positive Cases J and R, where the damage caused by the bacterium was not a determinant factor in ulceration. The hypersecretion of gastric acid in Cases J and R suggests the patients were severely impacted by stress and may result in bleeding. In these two cases, H. pylori eradication were not likely to prevent the relapse88,89. It is more common to identify cases similar to Cases G and I in clinical patients, whereas Cases D, F, J and R occur less frequently, which explains the dramatic decrease of relapse after H. pylori eradication90.
Discussion
Although 13 theories have been proposed, the pathogenesis of duodenal ulcer remains elusive. Guided by the CCR with its accompanying methodologies, Theory of Nodes pinpointed the etiology of peptic ulcers from historical data and proposed a psychopathological mechanism, which elucidated 7 characteristics and 42 observations/phenomena of duodenal ulcer (Supplementary Table S2-S6). Unequivocally, a full understanding of the pathogenesis is indispensable for the development of strategies for a complete cure of the disease without relapse. Herein it is the application of the CCR with its accompanying methodologies that garners Theory of Nodes unprecedented insights into duodenal ulcers.
The psychopathological mechanism elucidated herein indicates that duodenal ulcer is a chronic disease associated with the individual’s life experiences/daily behaviors, and multiple psycho-neuro-endocrine organs are involved. Thus, stress-induced duodenal ulcer is hardly reproduced in animal models36 due to short lifespans. This mechanism also elucidated that the crux of duodenal ulcer issue is the hyperplasia and hypertrophy of gastrin and parietal cells induced by chronic stress. Therefore, neither anti-acid nor anti-H. pylori treatments can prevent the relapse of the disease17, whereas stress management is essential for a complete cure without relapse. Based on the mechanism elucidated herein, Theory of Nodes recommends two levels of stress management for duodenal ulcer disease prevention. At the individual level, healthy habits and lifestyles improve both physical and mental well-being. To reduce stress from daily life, an individual should try her/ his best to maintain harmonious family, social, and working environments. At the societal level, creating a positive and healthy environment is extremely important to cultivate healthy dispositions. This requires governments to lead and participate on all levels by fulfilling their administrative roles and promoting the harmonies of social, natural, and working environments to their citizens. These efforts will maximally reduce the chronic stress induced by social competitions and conflicts. Eventually, the morbidity and mortality rates of peptic ulcers may decrease to a minimal level.
Apparently, the pathogenesis of duodenal ulcers has never been fully understood before, primarily because a universal CCR has yet to be established and therefore, there is no benchmark for etiological factors. Consequently, modern medical doctors changed their research direction from time to time, resulting in the 13 etiological theories over the centuries. In that case, it was not surprising that the 3 local aggressive factors, gastric acid, H. pylori, and NSAIDs, were considered etiological factors one after another, causing multiple controversies and mysteries in peptic ulcer research. In contrast, guided by the CCR, Theory of Nodes pinpointed the cause of peptic ulcers from historical data, and combined Psychosomatic Theory and Stress Theory into a complete etiology of the disease. This new etiology elucidated that all the 3 local aggressive factors are not etiological factors, but risk factors playing a role in only the late phase of the disease. As a result, 7 characteristics and 42 observations/phenomena of duodenal ulcers, most of which have never been understood before, were explicitly elucidated. The effectiveness indicates that Theory of Nodes may have definitely identified the etiology of duodenal ulcers for the first time in history. Obviously, without the CCR, modern research on all other diseases is similar to the peptic ulcer research and thus, to this day, no disease has been fully explained and the majority of diseases, such as cancer and AIDS, remain incurable. Herein the first application of the CCR identified the etiology of a model disease, suggesting it may be widely applied to identify the etiology of any disease.
Although Psychosomatic Theory and Stress Theory have discovered the real cause of peptic ulcers for 70 years, they still could not explain the pathogenesis of peptic ulcers. Theory of Nodes demonstrated that the methodological concepts derived from the CCR, Integral Perspective and Superposition Mechanism, are indispensable for the data analyses. Without the two concepts, much invaluable historical data is deemed outdated and remains unanalyzed in modern medicine. For example, the discovery of H. pylori overshadowed all the other 4 major etiological theories in history, Psychosomatic Theory, Stress Theory, Nerve Theory, and ‘No Acid, No Ulcer’. Interestingly, the application of Integral Perspective in Theory of Nodes pulled all these 4 theories from the shadow as each of them did make important discoveries and proved useful for a full understanding of duodenal ulcers. In addition, Superposition Mechanism superposed the corrosive effects of the local aggressive factors into a combinatorial force, thereby elucidating all the clinical, epidemiological, and laboratory observations of duodenal ulcers, as well as the roles of gastric acid, H. pylori, and NSAIDs in the disease. The research on all other diseases is in the same scenario, indicating that the wide application of these methodological concepts may allow us gain unprecedented insights for any disease.
Conclusion
Duodenal ulcer is a psychosomatic disease triggered by psychological stress, where gastric acid, H. pylori, and NSAIDs play a role in only the late phase of ulcerations, exacerbating clinical symptoms and increasing morbidity/mortality rates. The hyperplasia and hypertrophy of parietal and gastrin cells in the stomach induced by chronic stress potentiate the individual’s response to psychological stress, resulting in the hypersecretion of gastric acid and eventually, duodenal ulceration. This psychopathological mechanism elucidated 7 characteristics and 42 observations/phenomena of duodenal ulcers, suggesting stress management is essential for a complete cure of the disease without relapse. The validity showcased herein indicates that the CCR with its accompanying methodologies may be applied to understand the pathogenesis of any disease, potentially leading to novel insights into the disease.
Acknowledgements
Special thanks to Katelynn J. Rowe, who contributed time and effort to challenge the ideas, optimize the structure, and enrich the contents of the article. I would like to thank Douglas Rowe, Dr. Jonathan Weldrick, and Angela Haworth for draft revisions. I would also like to thank Dr. Xiao Xiang, Stephen Holland, Emily Freeman, and Dr. Ashok Kumar for their constructive comments. I am very grateful to Dr. Wuqiang Zhu for his assistance in literature search.
Ethics Statement
This study was conducted with integrity, fidelity, honesty, and did not involve any human or animal specimen.
Funding Statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Data Availability Statement
All the supporting data in this article are published papers or books, or in the supplementary materials.
Supplemental Materials
The supplementary materials include 6 tables in a PDF document.
ORCID: Simon Xin Min Dong https://orcid.org/0000-0003-0073-7216
References
- Albaqawi AS, El-Fetoh NMA, Alanazi RF, et al. Profile of peptic ulcer disease and its risk factors in Arar, Northern Saudi Arabia. Electron 2017;9 (11):5740-5745.
- FatoviÄ-FerenÄiÄ S, BaniÄ M. No acid, no ulcer: Dragutin (Carl) Schwarz (1868-1917), the man ahead of his time. Dig Dis. 2011; 29 (5): 507-
- von Bergmann Ulcus duodeni und vegetatives nerve system. Berl Klin Wchnscher. 1913; 50: 2374.
- Wolowitz Oral involvement in peptic ulcer. J. Consult. Psychol. 1967; 31: 418–419.
- Selye The physiology and pathology of exposure to stress. Acta. 1950.
- Dong SXM, Chang CCY, Rowe KJ. A collection of the etiological theories, characteristics, and observations/phenomena of peptic ulcers in existing data. Data Br. 2018; 19: 1058–1067.
- Kuang, Peptic Ulcer Diseases. People’s Medical Publishing House. 1990.
- Marshall Peptic Ulcer: An Infectious Disease? Hosp. Pract. 1987; 22: 87–96.
- Ford AC, Talley NJ. Head to Head: Does Helicobacter pylori really cause duodenal ulcers? BMJ. 2009; 339: b2784.
- Hobsley M, Tovey FI, Bardhan KD, et al. Head to Head: Does Helicobacter pylori really cause duodenal ulcers? BMJ. 2009; 339: b2788.
- Record CO, Rubin PC. Controversies in Management: Helicobacter pylori is not the causative agent. BMJ. 1994; 309: 1571–1572.
- Kate V, Ananthakrishnan N, Tovey Is Helicobacter pylori Infection the Primary Cause of Duodenal Ulceration or a Secondary Factor? A Review of the Evidence. Gastroenterol. Res. Pract. 2013.
- Tovey FI, Hobsley Review: is Helicobacter pylori the primary cause of duodenal ulceration? J. Gastroenterol. Hepatol. 1999; 14: 1053–1056.
- Iijima K, Kanno T, Koike T, et T. Helicobacter pylori-negative, non- steroidal anti-inflammatory drug: Negative idiopathic ulcers in Asia. World J. Gastroenterol. 2014; 20: 706.
- Gisbert JP, Calvet X. Review article: Helicobacter pylori-negative duodenal ulcer Aliment. Pharmacol. Ther. 2009; 30: 791–815.
- Kato S. The prevalence of Helicobacter pylori in Japanese children with gastritis or peptic ulcer J. Gastroenterol. 2004; 39: 734– 738.
- Wong GL, Wong VW, Chan Y, et al. High Incidence of Mortality and Recurrent Bleeding in Patients With Helicobacter pylori-Negative Idiopathic Bleeding Ulcers. Gastroenterology. 2009; 137: 525–531.
- Musumba C, Pritchard DM, Pirmohamed M. Review article: cellular and molecular mechanisms of NSAID-induced peptic Aliment. Pharmacol. Ther. 2009; 30: 517–531.
- Dong SXM, Chang Philosophical Principles of Life Science. Wunan Culture Enterprise. 2012.
- Wretmark The peptic ulcer individual; a study in heredity, physique, and personality. Acta Psychiatr. Neurol. Scand. Suppl. 1953; 84: 1–183.
- Doll R, Jones FA, Buckatzsch Occupational Factors in the Aetiology of Gastric and Duodenal Ulcers, with an Estimate of their Incidence in the General Population. Br. J. Ind. Med. 1951; 8: 308–309.
- Feldman M, Weinberg Healing of peptic ulcer. Am. J. Dig. Dis. 1951; 18: 295–6.
- Feldman M, Walker P, Green JL, et al. Life events stress and psychosocial factors in men with peptic ulcer disease: a multidimensional case- controlled study. Gastroenterology. 1986; 91: 1370–9.
- Levenstein Psychologic predictors of duodenal ulcer healing. J. Clin. Gastroenterol. 1996; 22: 84–89.
- Carey G, DiLalla Personality and psychopathology: Genetic perspectives. J. Abnorm. Psychol. 1994; 103: 32–43.
- Tennant C, Goulston K, Langeluddecke P. Psychological correlates of gastric and duodenal ulcer Psychol. Med. 1986; 16: 365–371.
- Magni G, Salmi A, Paterlini A, et Psychological distress in duodenal ulcer and acute gastroduodenitis. Dig. Dis. Sci. 1982; 27: 1081–1084.
- Levenstein Stress and peptic ulcer: life beyond helicobacter. Bmj. 1998; 316: 538–541.
- Levenstein S, Prantera C, Varvo V, et al. Life events, personality, and physical risk factors in recent-onset duodenal ulcer: a preliminary J. Clin. Gastroenterol. 1992; 14: 203–210.
- Bruce Overmier J, Murison Anxiety and helplessness in the face of stress predisposes, precipitates, and sustains gastric ulceration. Behav. Brain Res. 2000; 110: 161–174.
- Yeomans The ulcer sleuths: The search for the cause of peptic ulcers. J. Gastroenterol. Hepatol. 2011; 26: 35–41.
- Bresnick WH, Rask-Madsen C, Hogan DL, et al. The Effect of Acute Emotional Stress on Gastric Acid Secretion in Normal Subjects and Duodenal Ulcer Patients. J. Clin. Gastroenterol. 1993; 17: 117–122.
- Peters MN, Richardson Stressful Life Events, Acid Hypersecretion, and Ulcer Disease. Gastroenterology. 1983; 84: 114–119.
- Levenstein S, Jacobsen RK, Rosenstock S, et al. Mental vulnerability, Helicobacter pylori, and incidence of hospital-diagnosed peptic ulcer over 28 years in a population-based cohort. Scand. J. Gastroenterol. 2017; 52: 1–8.
- Miner P. Review article: Relief of symptoms in gastric acid-related diseases-correlation with acid suppression in rabeprazole Aliment. Pharmacol. Ther. 2004; 20 Suppl 6: 20–29.
- Glavin GB, et al. The neurobiology of stress ulcers. Brain Res. Rev. 1991; 16: 301–343.
- Jones MP. The role of psychosocial factors in peptic ulcer disease: Beyond Helicobacter pylori and J. Psychosom. Res. 2006; 60: 407–412.
- Furuta T, Baba S, Takashima M, et al. Effect of Helicobacter pylori Infection on Gastric Juice pH. Scand. J. Gastroenterol. 1998; 33: 357–
- Huerta-Franco MR. Effects of occupational stress on the gastrointestinal tract. World J. Gastrointest. Pathophysiol. 2013; 4:
- Kurata JH, Nogawa AN, Abbey DE, et al. A prospective study of risk for peptic ulcer disease in seventh-day adventists. Gastroenterology. 1992; 102: 902–909.
- Ellard K, Beaurepaire J, Jones M, et al. Acute and chronic stress in duodenal ulcer disease. Gastroenterology. 1990; 99: 1628–1632.
- Menzel C, Dennenmoser F, Reese Feeling stressed and ugly? Leave the city and visit nature! an experiment on self-and other-perceived stress and attractiveness levels. Int. J. Environ. Res. Public Health. 2020; 17: 1–15.
- Kennedy DP, Adolphs Stress and the city. Nature. 2011; 474: 452–453.
- Rauws EAJJ, Tytgat GNJJ. Helicobacter pylori in duodenal and gastric ulcer disease. Baillieres. Clin. Gastroenterol. 1995; 9: 529–547.
- Ramakrishnan K, Salinas Peptic Ulcer Disease: Am. Fam. Physician. 2007; 76: 1005–1012.
- Dragstedt Peptic ulcer: An Abnormality in Gastric Secretion. Am. J. Surg. 1969; 117: 143–156.
- Ganguli PC, Pearse AGE, Polak J, et Antral-Gastrin-Cell hyperplasia in peptic ulcer disease. Lancet. 1974; 303: 583–586.
- Nazirov FG, Nishanov MF, Bozorov NE, et al. Duodenal Ulcer Complicated by Piloroduodenal Stenosis : Technical and Tactical Approaches of Treatment. Am. J. Med. Med. Sci. 2020; 10: 96–101.
- Earlam A Computerized Questionnaire Analysis of Duodenal Ulcer Symptoms. Gastroenterology. 1976; 71: 314–317.
- Moffitt Symposium on Duodenal Ulcer: 1. Medical Aspects. Can. Med. Assoc. J. 1926; 16: 1044–50.
- Stolte M, Meining A, Seifert E, et Treatment with lansoprazole also induces hypertrophy of the parietal cells of the stomach. Pathol. Res. Pract. 2000; 196: 10–14.
- Mazzacca G, Cascione F, Budillon G, et Parietal cell hyperplasia induced by long-term administration of antacids to rats. Gut. 1978; 19: 798–801.
- Til HP, Woutersen RA, Feron VJ, et Two-year drinking-water study of formaldehyde in rats. Food Chem. Toxicol. 1989; 27: 77–87.
- Dragstedt LR. Role of the vagus nerves in the physiology of gastric Am. J. Surg. 1969; 117: 813–821.
- Håkanson R, Böttcher G, Sundler F, et al. Activation and hyperplasia of gastrin and enterochromaffin-like cells in the stomach. Digestio. 1986; 35 Suppl 1: 23–41.
- Ulrich-Lai YM, et al. Chronic stress induces adrenal hyperplasia and hypertrophy in a subregion-specific manner. AJP Endocrinol. Metab. 2006; 291: E965-E973.
- Delaney JP, Michel HM, Bonsack ME, et Adrenal Corticosteroids Cause Gastrin Cell Hyperplasia. Gastroenterology. 1979; 76: 913–916.
- Guida PM, Todd JE, Moore SW, et al. Zollinger-ellison syndrome with interesting variations. Am. J. Surg. 1966; 112: 807–817.
- Rogers Primary Hypertrophy and Hyperplasia of the Parathyroid Glands Associated with Duodenal Ulcer. Arch. Intern. Med. 1947; 79: 307.
- Moreau JF. Parathyroid Ultrasonography of the Neck. 51–63; Springer Berlin Heidelberg, 1987.
- Susser M, Stein Civilization and Peptic Ulcer. Lancet. 1962; 279: 116–119.
- Christodoulou GN, Gargoulas A, Papaloukas A, et al. Peptic Ulcer in Psychother. Psychosom. 1979; 32: 297–301.
- Blair AJ, Feldman M, Barnett C, et al. Detailed comparison of basal and food-stimulated gastric acid secretion rates and serum gastrin concentrations in duodenal ulcer patients and normal J. Clin. Invest. 1987; 79: 582–587.
- Mcintosh JH, Nasiry RW, Frydman M, et The Personality Pattern of Patients with Chronic Peptic Ulcer. Scand. J. Gastroenterol. 1983; 18: 945–950.
- Kirsner JB, Palmer WL. Seminars on gastrointestinal physiology: The problem of peptic Am. J. Med. 1952; 13: 615–639.
- Szabo S. Duodenal ulcer disease animal model: cysteamine-induced acute and chronic duodenal ulcer in the Rat. Am. J. Pathol. 1978; 93: 273–276.
- Li H, Kalies I, Mellgård B, et al. A Rat Model of Chronic Helicobacter pylori Infection: Studies of Epithelial Cell Turnover and Gastric Ulcer Scand. J. Gastroenterol. 1998; 33: 370–378.
- Graham DY, Yamaoka pylori and cagA: Relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter. 1998; 3: 145–151.
- Huang JQ, Sridhar S, Hunt RH. Role of Helicobacter pylori infection and non-steroidal anti-inflammatory drugs in peptic-ulcer disease: A meta-analysis. Lancet. 2002; 359: 14–22.
- Brzozowski T, Konturek PC, Sliwowski Z, et al. Interaction of nonsteroidal anti-inflammatory drugs (NSAID) with Helicobacter pylori in the stomach of humans and experimental J. Physiol. Pharmacol. 2006; 57: 67–79.
- Konturek PC, Konturek SJ, CzeÅnikiewicz M, et al. Interaction of Helicobacter pylori (Hp) and nonsteroidal anti-inflammatory drugs (NSAID) on gastric mucosa and risk of ulcerations. Med. Sci. Monit. 2002; 8: 197–209.
- Yamaoka Y, Kodama T, Kita M, et al. Relation between clinical presentation, Helicobacter pylori density, interleukin 1β and 8 production, and cagA status. Gut. 1999; 45: 804–811.
- Marshall BJ, Goodwin CS, Warren JR, et al. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter Lancet (London, England). 1988; 2: 1437–42.
- Weel JF, van der Hulst RW, Gerrits Y, et al. The Interrelationship between Cytotoxin-Associated Gene A, Vacuolating Cytotoxin, and Helicobacter pylori-Related Diseases. J. Infect. Dis. 1996; 173: 1171–
- Woo HJ, Yang JY, Lee MH, et al. Inhibitory Effects of β-Caryophyllene on Helicobacter pylori Infection In Vitro and In Vivo. Int. J. Mol. Sci. 2020; 21: 1008.
- Elitsur Y, Lawrence Non-Helicobacter pylori related duodenal ulcer disease in children. Helicobacter. 2001; 6: 239–243.
- Roma E, Panayiotou J, Kafritsa Y, et Upper gastrointestinal disease, Helicobacter pylori and recurrent abdominal pain. Acta Paediatr. 1999; 88: 598–601.
- Quan C, Talley NJ. Management of peptic ulcer disease not related to Helicobacter pylori or Am. J. Gastroenterol. 2002; 97: 2950– 2961.
- Pilotto A, Leandro G, Di Mario F, et al. Role of Helicobacter pylori infection on upper gastrointestinal bleeding in the elderly: a case- control study. Dig. Dis. Sci. 1997; 42: 586–591.
- Parsonnet Helicobacter pylori: the size of the problem. Gut. 1998; 43: S6–S9.
- Katz Once an ulcer, always an ulcer? Am. J. Gastroenterol. 1994; 89: 808–809.
- Miller JP, Faragher Relapse of duodenal ulcer: does it matter which drug is used in initial treatment. BMJ. 1986; 293: 1117–1118.
- Sivri Trends in peptic ulcer pharmacotherapy. Fundam. Clin. Pharmacol. 2004; 18: 23–31.
- Leung WK, Graham Rescue therapy for Helicobacter pylori. Curr. Treat.Options Gastroenterol. 2002; 5: 133–138.
- Gisbert JP. Rescue Therapy for Helicobacter pylori Infection 2012. Res. Pract. 2012.
- Laine Effect of Proton-Pump Inhibitor Therapy on Diagnostic Testing for Helicobacter pylori. Ann. Intern. Med. 1998; 129: 547.
- Freston Role of proton pump inhibitors in non-H. pylori-related ulcers. Aliment. Pharmacol. Ther. 2001; 15: 2–5.
- Niv H pylori recurrence after successful eradication. World J. Gastroenterol. 2008; 14: 1477.
- Zullo A, Hassan C, Cristofari F, et al. Effects of Helicobacter pylori Eradication on Early Stage Gastric Mucosa–Associated Lymphoid Tissue Lymphoma. Clin. Gastroenterol. Hepatol. 2010; 8: 105–110.
- Malfertheiner P, Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007; 56: 772–781.
Supplementary Materials
The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers
Table of Contents
|
Table S1: List of 6 articles to explain all the 15 characteristics and 81 observations/phenomena of peptic ulcers |
14 |
|
Table S2: Index of 7 elucidated characteristics of peptic ulcers |
14 |
|
Table S3: Index of 6 elucidated duodenal ulcer-related observations/phenomena |
15 |
|
Table S4: Index of elucidated gastric ulcer-related observations/phenomena |
15 |
|
Table S5: Index of 11 elucidated both gastric and duodenal ulcer-related observations/phenomena |
16 |
|
Table S6: Index of 25 elucidated H. pylori-related observations/phenomena |
18 |
Table S1: List of 6 articles to explain all the 15 characteristics and 81 observations/phenomena of peptic ulcers
|
Article |
Title |
|
A1* |
The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers |
|
A2 |
A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers |
|
A3 |
Novel Data Analyses Explain the Birth-Cohort Phenomenon of Peptic Ulcers |
|
A4 |
Novel Data Analyses Explain the Seasonal Variation of Peptic Ulcers |
|
A5 |
Painting a Complete Picture of the Pathogenesis of Peptic Ulcers |
|
A6 |
Novel Data Analyses Address the African Enigma and the Controversies Surrounding the Roles of Helicobacter Pylori in Peptic Ulcers |
Note: 1. A1: Article 1. 2. * This Article. 3. The 6 articles altogether explained all of the 15 major characteristics and 81 observations/
phenomena of peptic ulcers. 4. The order and titles of articles might be modified during publication process.
Table S2: Index of 7 elucidated characteristics of peptic ulcers
|
Classification |
Characteristics |
Explanation in the Article |
Article, Page, Column & Line # |
|
General (3) |
1) Genetic predisposition |
|
|
|
2) Etiology |
Peptic ulcers are not an infectious disease caused by the H. pylori infection, but a psychosomatic disease triggered by psychological stress. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
|
3) Epidemiology |
|
|
|
|
Clinical symptoms (6) |
4) Predilection sites |
|
|
|
5) Morphology |
|
|
|
|
6) Bleeding |
|
|
|
|
7) Perforation |
|
|
|
|
8) Relapse |
Clinical patients suffer relapses of peptic ulcers because neither anti-secretory nor anti-H. pylori therapy is an etio- logical treatment and thus, the hyperplasia and hypertro- phy of gastrin and parietal cells and the impact of stress have not been eliminated. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
|
9) Multiplicity |
|
|
|
|
Local aggressive factors (3) |
10) Gastric acid (in duodenal ulcer) |
The hypersecretion of gastric acid is an intermediate process of duodenal ulceration, suggesting it is not a cause of duodenal ulcers, but an effect of stress triggered by personality traits or life events. Nevertheless, the hypersecretion of gastric acid is a determinant factor in the late phase of duodenal ulceration, governing many characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-35. |
|
11) H. pylori (in duodenal ulcer) |
H. pylori infection is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left Column, Line 17; Article 1, Page 7, Right Column, Lines 34-41. |
|
|
12) NSAIDs (in duodenal ulcer) |
NSAIDs usage is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left column, Line 17; Article 1, Right Column, Page 7, Lines 34-41. |
|
|
Prognosis (3) |
13) Self-healing |
|
|
|
14) Effects of clinical treatments (Duodenal ulcer only) |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, but the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori- negative Cases D and F, or in the H. pylori-positive Cases J and R. Cases like Cases D, F, J and R explains a dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
|
15) Hospitalization rates, morbidity, and mortality (Duodenal ulcer only) |
Neither H. pylori infection nor NSAIDs usage is an etio- logical factor. Both play a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symp- toms and increasing clinical morbidity and mortality rates. |
Article 1, Page 7, Right Column, Lines 34-41. |
Note: The blank will be filled in other articles of the series.
Table S3: Index of 6 elucidated duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
1. No Acid, No Ulcer (True statement for duodenal ulcer). |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDS. |
Article 1, Page 5, Right Column, Lines 28-34. |
|
2. The role of gastric acid in the pathogenesis of duodenal ulcer is further supported by the relief of pain observed after neutralization or buffering of gastric contents with alkali or food. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors. Thus, neutralization or buffering of gastric contents with alkali or food results in the relief of pain in duodenal ulcer patients. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
3. Doll and Jones’ survey suggested a positive correlation between stressful occupations and duodenal ulcer, a decreased incidence of ulcer among agricultural workers. |
Psychosomatic factors such as hypochondriasis, a negative perception of life events, dependency, and lowered self- confidence, made ulcer patients more susceptible to stress than controls. |
Article 1, Page 3, Right Column, Line 36-Page 4, Left Column, Line 9. |
|
4. Studies suggest that severe anxiety caused acid hypersecretion which, in turn, contributed to ulceration and symptoms. The fact that acid hypersecretion and symptoms abated with alleviation of stress supports this hypothesis. |
The hypersecretion of gastric acid is triggered by the perception of stress via vagus nerves, and the hyperplasia and hypertrophy of gastrin and parietal cells in the early phase significantly potentiated the individual’s response to life events. |
Article 1, Page 5, Left Column, Lines 37-43. |
|
5. Rates of recurrence in patients whose initial ulcers healed during conventional anti-secretory therapy range from 60 to 100 percent per year. |
Neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’ |
Article 1, Page 8, Right Column, Lines 7-14. |
|
6. Duodenal ulcer had higher incidence in large cities compared to rural areas in Africa since the 1950’s. |
Life in large cities is more competitive and stressful than in rural areas. |
Article 1, Page 4, Left Column, Lines 9-12. |
Table S4: Index of elucidated gastric ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
7. No Acid, No Ulcer (wrong statements for gastric ulcers). |
|
|
|
8. In contrast to patients with duodenal ulcer, most patients with gastric ulcer are normo- secretors or hypo-secretors. Decreased acid-peptic activity in these patients suggests impaired mucosal defence. |
|
|
|
9. Gastric ulcer is a sharply circumscribed loss of tissue involving the mucosa, submucosa, and muscular layer and a characteristic “punch out” appearance with clean edges, as if it were cut by a knife. |
|
|
|
10. Gastric ulcers can be induced only in 8-30% of mouse models. |
|
|
|
11. Gastric ulceration begin in the mucosa and extend into the wall of the stomach. |
|
|
|
12. Stress-related gastric lesions are ‘brain-driven’ events that may be more effectively managed through central manipulations than by altering local, gastric factors. For example, stimulation or lesions of the central nucleus of the amygdala produced or reduced gastric ulcers, respectively. |
|
|
|
13. Development of gastric ulcers elicited by cold stress was significantly decreased by i.p. pre-treatment with EDTA or a-methyl tyrosine, which depleted neurotransmitters. Gastric ulcers were significantly increased by pre-treatment with CaCl2. |
|
|
|
14. The predilection sites of gastric ulcers are gastric antrum and lesser curvature. |
|
|
|
15. Vulnerability to gastric ulceration is modulated by psychologically meaningful experiences. Repeated stress of the same type generally, but not exclusively, provides some degreeof protection against ulcer during the second or later exposures. |
|
|
Note: Although no observation/phenomenon of gastric ulcer was explained in this first article, for the integrity of all the 15 major characteristics and 81 observations/phenomenaof peptic ulcers, it is still necessary to retain the observations/phenomena of gastric ulcer here. This table will be filled in the second article, which focuses exclusively on the topic of gastric ulcer.
Table S5: Index of 11 elucidated both gastric and duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page,Column & Line # |
|
16. The pathogenesis of NSAID-induced peptic ulcers is complex andmulti-factorial. |
|
|
|
17. 14% of patients taking NSAIDschronically can be found to have lesions described as gastric ulcers and 10% have lesions describes as duodenal ulcers. |
|
|
|
18. Birth-cohort Phenomenon: the mortality rate of gastric ulcers in England and Wales increased at the beginning of the 20th century, reached a peak and then began to fallin the early 1950s. They also found similar trends for duodenal ulcers but followed approximately five years behind. |
|
|
|
19. Once an ulcer, always an ulcer. |
Clinical patients suffer relapses of peptic ulcers because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy ofgastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’ |
Article 1, Page 8, Right Column, Lines 7-14. |
|
20. Seasonal occurrence of pepticulcer diseases. |
|
|
|
21. Patients free of ulcer distress forlong periods of time were subjectedto emotional trauma and feelings ofinsecurity during the symptom-free intervals. |
|
|
|
22. Investigations of the effects ofperceived stress on physiological parameters are scarce and the findings are often conflicting. |
Questionnaire-based epidemiological surveysmay have discounted many chronic stressors during peptic ulcer research, and that the essential methodology to study psychosocial factors (the abstract essence of the human body) have not been established in modern medicine. |
Article 1, Page 5, Left Column, Line 44- Page 5, Right Column, Line 13. |
|
23. There is no definitive study proving a causal relationship between psychological stress and the development of ulcer disease. |
Without the CCR, there is no benchmark to identify the cause of ulcer disease. without the methodological concepts derived from the CCR, much invaluable historical data is deemed outdated and remains unanalyzed. |
Article 1, Discussion, Page 9, Left Column, Lines 43-53; Article 1, Discussion, Page 9, Right Column, Lines 19-43. |
|
24. Feldman’s multidimensional case-controlled study found that ulcer patients exhib- ited significantly more emotional distress in the form of depression and anxiety. |
|
|
|
Hypochondriasis, a negative perception of their life events, dependency, and lowered self-confidence were the four variables that best discriminated ulcer patients from controls. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individ- uals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
25. Peptic ulcers are a rare disease in childhood. |
|
|
|
26. Although gastric ulcer and duodenal ulcer share something in common, they are believed to be differ- ent diseases. |
|
|
|
27. The final stage of ulceration is a corrosive rather than an infectious process. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors, including gastric acid and pepsin, H. pylori, mechanical abrasion, and chemical erosion from medications such as NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
28. The gastric acid secretion of duodenal ulcer pa- tients is much higher than a normal person, but only 7–8.5% of the duodenal ulcer patients are suffering from gastric ulcer simultaneously. |
|
|
|
29. Severe emotional stress may contribute to ulcer perforation and bleeding in some patients. |
|
|
|
30. Many uncomplicated lesions heal in spite of the presence of acid gastric content, as shown by the “spontaneous” remissions of the disease and by the healed scars found at x-ray and at autopsy; however, the healing of peptic ulcer is much more rapid when the lesion is protected from the action of acid gastric juice. |
|
|
|
31. Autopsy reports showed: 20%-29% of males and 11%-18% of females were found to have suffered from ulcers in the past or present. |
|
|
|
32. It is believed that, not only should the prognosis and assessment of ulcer have mental assessment, but the treatment without mind adjustment is also incomplete. |
|
|
|
33. Peptic ulcer patients may have “ulcer personality”, such as immaturity, impulsivity, and feelings of social isolation and alienation. |
|
|
|
34. In a 2-year study of Pima Indians, Hesse did not find any peptic ulcer disease. |
|
|
|
35. In contrast to Pima Indians, 10% of Caucasians develop peptic ulcers. |
|
|
|
36. To date, no consistent pattern of factors, in either host or organism, has been identified that successfully predicts which infected persons will subsequently have ulcer disease. |
|
|
|
37. The relationship between life events stress, psychological factors and peptic ulcer diseases is not clearly established at the present time and warrants further study. |
Without the CCR, there is no benchmark to identify the cause of disease. As a result, no disease has been fully understood. Without the CCR, the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. |
Article 1, Discussion, Page 9, Left Column, Lines 43-53; Article 1, Discussion, Page 9, Right Column, Lines 19-43. |
|
38. Richard emphasized the different aetiology of gastric and duodenal ulcers and persons with gastric and duodenal ulcers differ epidemiologically, behaviourally, and genetically. |
|
|
|
39. Gastric ulcer was more frequent than duodenal ulcer, 4G:1D in 1900 versus 10D:1G currently. More women than men had the disease, but now it has become reversed; from 3F:1M to 4M:1F for gastric ulcer and 10M:1F for duodenal ulcer. |
|
|
|
40. Stress ulcers in the rat are primarily gastric rather than duodenal, the latter typically requiring additional artificial chemical potentiation (e.g., histamine). |
It may take ~5 years to induce the hyperplasia and hypertrophy in the human body. As a result, it is hard to duplicate this chronic pathophysiological process in the lab, thereby making it difficult to establish animal models for stress-induced duodenal ulcers. |
Article 1, Page 5, Left Column, Lines 14-20; Article 1, Discussion, Page 9, Left Column, Lines 15-20. |
|
41. Many ulcer patients and some physicians believe that symptomatic exacerbations of peptic ulcer disease occur during or shortly after stressful events. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
42. Mental disorders (or stress) are associated with increased rates of peptic ulcer diseases. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors, which focuses more on the impact of mental health related to past life experience, made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
43. The spontaneous remissions andrelapses of peptic ulcers have neverbeen explained. |
Clinical patients suffer the relapse of pepticulcers, because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the impact of stress caused by personality traits or negative lifeevents has not been eliminated. |
Article 1, Page 8, Right Column, Lines 7-14; |
|
44. The pathophysiology of pepticulcer has centred on an imbalancebetween aggressive and protective factors. |
|
Article 1, Discussion, Page 9, Left Column, Lines 15-26. |
|
45. No single theory in history couldfully explain the pathogenesis of peptic ulcers. |
Each of the single theory focused on only onearea of the human body, and there is no holistic review of peptic ulcers before. |
Article 1, Page |
Table S6: Index of 25 elucidated H. pylori-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
46. African Enigma: The H. pylori infection rate is high (close to 100%) throughout Africa, but the prevalence of duodenal ulcer varied in different parts of the continent. |
|
|
|
47. Only the presence of duodenal ulcers, and not gastric ulcers, was associated with increasing H. pylori density. The association between gastric ulcers and H. pylori infection is less clear. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. Cases B to J explain why H. pylori density is associated with the morbidity rate of duodenal ulcers. ‘The association between gastric ulcers and H. pylori infection is less clear’ will be explained in A2, which focuses on the pathogenesis of gastric ulcer. |
Article 1, Page 7, Right Column, Lines 34-48. |
|
48. Only 27% of symptomatic children with peptic ulcers were H. pylori positive. |
|
|
|
49. 48% of patients developed ulcers within six months of healing, but the re-infection rate after eradication was very low (<2%). |
|
|
|
50. In developing countries with uniformly high prevalence of H. pylori infection, there are marked regional differences in the prevalence of duodenal ulcers, which could not be explained by the more toxic CagA and VacA H. pylori strains. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
51. In the countries with low prevalence of H. pylori, 30%-40% or more of duodenal ulcer patients are H. pylori-negative, and the absence of H. pylori infection in early cases of duodenal ulcers was also reported. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration. Cases D, F, L, and N support the finding that in some countries, 30%-40% of duodenal ulcer 386 patients were H. pylori-negative and explain a clinical observation that up to 35% of 387 infected patients failed to respond to standard anti-H. pylori therapy. |
Article 1, Page 8, Left Column, Lines 2-16; Article 1, Page 8, Right Column, Lines 19-27. |
|
52. The role of H. pylori in peptic ulcers is controversial. |
Without the CCR, there is no benchmark to identify the cause of disease, and the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. No longer controversial after the application of the CCR. |
Article 1, Discussion, Page 9, Left Column, Lines 43-53; Article 1, Discussion, Page 9, Right Column, Lines 19-43. |
|
53. ‘H. pylori is the most important aetiological factor so far described for duodenal ulcer’. |
This is a wrong statement. The hyper-secretion of gastric acid is a determinant factor in the late phase of duodenal ulceration; Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, suggesting it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duodenal ulcers. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
54. How H. pylori infection can lead to ulceration is unknown. |
This statement is based on a wrong assumption. Without the hypersecretion of gastric acid, the corrosive intensity caused by either H. pylori or NSAIDs could not reach the threshold of ulceration. H. pylori alone cannot lead to ulceration and thus, the etiology based on H. pylori infection would never be able to explain peptic ulcerations. |
Article 1, Page 7, Right Column, Lines 44-53. |
|
55. No H. pylori, No Ulcer; peptic ulcer is an infectious disease. |
These are wrong statements. Neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 38-48. |
|
56. In spite of a high prevalence of H. pylori infection worldwide, the incidence of duodenal ulcer disease in both adults and children is low in comparison. |
Case B is applicable to most H. pylori infected individuals, but only those also impacted by the hyper-secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. |
Article 1, Page 8, Left Column, Lines 17-23. |
|
57. Kato and colleagues’ retrospective analysis found that H. pylori prevalence in gastric ulcer did not reach 50%; they concluded while H. pylori infection appears to be a risk factor in gastric ulcer, other causes are responsible for most cases. Only 56-96% of gastric ulcer patients are H. pylori-positive, so other factors must be involved. |
|
|
|
58. Despite the fall in prevalence of H. pylori infection, the attributable risk of H. pylori infection in peptic ulcer disease has not changed. |
|
|
|
59. There was a significantly higher incidence of idiopathic duodenal ulcers in the younger generation. |
|
|
|
60. There are basically three different types of peptic ulcer: H. pylori-related peptic ulcer; NSAID-related peptic ulcer; and non-H. pylori, non-NSAID ulcer. |
This classification is because the cause of peptic ulcers has never been not identified in modern medicine. This classification overlooks the primary/decisive factor in the occurrence of duodenal ulcers, the hypersecretion of gastric acid. |
Article 1, Page 8, Right Column, Lines 14-18. |
|
61. A relatively isolated group of Australian aboriginals have virtually no H. pylori infection and hardly any peptic ulcer disease. |
|
|
|
62. Up to 20% of patients with ulcers suffer a relapse of ulcer disease despite successful eradication of their infections, suggesting that H. pylori was not the cause of their original ulcers. |
Cases D and F were caused simply by the hypersecretion of gastric acid due to psychological stress, which explain 20%-40% of patients with idiopathic ulcers (H. pylori- negative and non-NSAIDs user) and the eradication of H. pylori can not prevent the relapse of these cases. |
Article 1, Page 8, Left Column, Lines 42-46. |
|
63. Difference in virulence of H. pylori strains (cag- and cag+) has been considered as a putative explanation as to why only a minority of infected population develop peptic ulcers. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA, cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
64. H. pylori infection in rats was successful and was accompanied by amild to moderate mucosal inflammation. After H. pylori inoculation, an ulcer was induced in the oxyntic mucosa of both infected and uninfected rats by exposing the serosal side to acetic acid. |
For those individuals with severe hyperplasia and hypertrophy of gastrin andparietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential forulceration. Therefore, duodenal ulcers mayoccur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating that gastric acid plays a more important role than H. pylori in duodenal ulcerations. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
65. More than 95 percent of patientswith duodenal ulcers and more than80 percent of patients with gastric ulcers are infected with H. pylori. |
|
|
|
66. The corresponding ulcer areas in the H. pylori-infected rats were significantly larger in the infected than in the uninfected rats, and ulcerhealing was delayed in the infected rats. Eliminating H. pylori accelerates the healing of ulcer. |
|
|
|
67. Eradication of H. pylori in gastriculcer patients has also been shown tobe associated with a significant reduction in ulcer relapse rate, compared with those who remain infected. |
|
|
|
68. Clinical data reported that the recurrence rate is as high as 74-80% in H. pylori positive group of duodenal ulcer patients who have healed, but the negative group is only 0-28%. The discrimination was remarkable. |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, which are representative of most clinical patients. However, the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori-negative Cases D and F, or in the H. pylori-positive Cases J and R, where the damage caused by the bacterium was not a determinant factor in ulceration. It is more common to identify cases similar to Cases G and I in clinical patients, whereas cases like Cases D, F, J and R occur less frequently, which explains the dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
69. A negative interaction between H. pylori and NSAIDs on duodenal ulcers suggests that H. pylori reduces the development of ulcers in NSAIDs users. |
H. pylori upregulates the expression of COX-2 and subsequently results in the biosynthesis of gastropro- tective prostaglandin, which in turn offsets the corrosive intensity of NSAIDs and thus is conducive to the healing of NSAIDs-induced ulcers, causing ‘H. pylori reduces the development of ulcers in NSAIDs users’. |
Article 1, Page 7, Left Column, Lines 46-52. |
|
70. ~20% of peptic ulcers in the Polish population are unrelated to H. pylori and NSAIDs use (idiopathic ulcers). |
For individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
71. The prevalence of H. pylori in patients with bleed- ing ulcers may be 15~20% lower than in patients with non-bleeding ulcers. |
Bleeding indicates patients are more likely to be seriously impacted by psychological stress with severe hyperplasia and hypertrophy of parietal and gastrin cells as Cases F and H. pylori infection is not essential for ulceration. In contrast, non-bleeding ulcer suggests the patients are more likely to be slightly impacted by stress with mild hyperplasia and hypertrophy, and H. pylori infection is essential to increase the total corrosive intensity for the induction of ulcers as Case G. As a result, clinical bleeding ulcer patients are more likely to be Case F without H. pylori and non-bleeding patients are more likely to be Case G with H. |
Article 1, Page 8, Left Column, Line 47-Right Column, Line 7. |
|
72. The eradication of H. pylori reduces the rate of re-bleeding in patients with ulcer disease. |
The eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 41-44. |
|
73. How H. pylori infection affects gastric acid secretion is still unclear. |
The hypersecretion of gastric acid is unrelated to any of the local aggressive factors, such as H. pylori infection, NSAIDs and other medications, but potentiated by the hyperplasia and hypertrophy of one or more endocrine organs and triggered by psychological stress due to personality traits or life events. Thus, ‘H. pylori infection affects gastric acid secretion’ is a wrong assumption. |
Article 1, Page 5, Right Column, Lines 20-35. |
|
74. The incidence of peptic ulcers was higher in H. pylori- infected patients than in the H. pylori-negative group. |
Since each of the 3 local aggressive factorspartially contributes to the corrosive intensity, and duodenal ulceration is causedby the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/ mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
75. Duodenal acid load determines whether H. pylori can cause duodenalulcer. |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 25-35. |
|
76. The increase in H. pylori density is related to the presence of duodenalulcer disease. |
Since each of the 3 local aggressive factorspartially contributes to the corrosive intensity, and duodenal ulceration is causedby the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/ mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
77. H. pylori-negative duodenal ulcers were associated with a poorer prognosis mainly because of a higherrate of ulcer and symptom relapse. |
To reach the ulceration threshold without the corrosive intensity from H. pylori, the hypersecretion of gastric acid needs to be higher in H. pylori-negative patients. The higher hypersecretion in Cases D and F indicates more severe negative impacts from psychosocial stress than in Cases G and I. Additionally, the damage from H. pylori can be relieved by antibiotics, as in Cases G and I, decreasing the corrosive intensity in these patients, whereas Cases D and F cannot achieve the same therapeutic effect. There- fore, there is a poorer prognosis and a higher relapse rate in H. pylori-negative patients. |
Article 1, Page 8, Left Column, Lines 31-41. |
|
78. When H. pylori persisted, 61% of duodenal ulcers healed and 84% relapsed. When H. pylori was cleared 92% of ulcers healed and only 21% relapsed during the 12 months follow-up period. |
Since each of the 3 local aggressive factors partially con- tributes to the corrosive intensity and duodenal ulceration is caused by the total corrosive intensity, the higher densi- ty of H. pylori, the higher total corrosive intensity. As a re- sult, H. pylori infection exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. In contrast, the eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 34-44. |
|
79. Jyotheeswaran and colleagues from greater Rochester, New York, reported a 48% prevalence of H. pylori-negative duodenal ulcers in white patients and 15% in non-white patients, with an overall negative prevalence of 39%. Parsonnet’s meta-analysis indicates the overall prevalence of H. pylori-negative duodenal ulcers is 40%. |
For those individuals with severe hyperplasia and hyper- trophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcer- ations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ul- cers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
80. A review by van der Voort and colleagues suggests that existing data are consistent with a causal role for H. pylori in stress ulcer formation. |
A statement originated from wrong etiology. ‘A causal role for H. pylori in stress ulcer’ indicates that without stress, H. pylori alone can not induce ulcer. Administering cysteamine or propionitrile, which effec- tively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duo- denal ulcer. Case B in Figure 2 is applicable to most H. pylori infected individuals, but only those also impacted by the hyper- secretions of gastric acid due to psychological stress (Case G) will have the chance to becomeulcer patients. That explained the wrong statement “a causal role for H. pylori in stress ulcer formation” |
Article 1, Page 5, Right Column, Lines 43-52. Article 1, Page 8, Left Column, Lines 17-25. |
|
81. Barry Marshall drank a concoction made from cultured H. pylori and came down with gastritisthat could be cured with antibiotics. |
|
|