
Painting a Complete Picture of the Pathogenesis of Peptic Ulcers
Simon Xin Min Dong
International Institute of Consciousness Science®, Vancouver, BC, Canada
Abstract
Peptic ulcers, including duodenal and gastric ulcers, were currently considered an infectious disease caused by Helicobacter pylori. However, this etiology cannot explain the major characteristics and observations/phenomena of the disease. To address the challenge, a Complex Causal Relationship with its accompanying methodologies was applied to analyze the existing data. Peptic ulcers were identified as a psychosomatic disease triggered by psychological stress, whereas Helicobacter pylori plays a secondary role in the late phase of peptic ulceration. This etiology addresses all the characteristics, observations/phenomena, controversies, and mysteries of peptic ulcers in a series of 6 articles. This third article discusses the etiology in-depth, painting a complete picture of the pathogenesis of peptic ulcers. The early phase is a long-term abstract psychopathological process, starting from early life when the impacts of multiple psychosomatic factors are transformed into hyperplasia and hypertrophy of gastrin and parietal cells and/or negative life-views via superposition mechanism. These pre-existing abnormalities potentiate the individual’s response to current psychological stress in the intermediate phase, resulting in hypersecretion of gastric acid and/or pre-ulcer lesions. The late phase is a corrosion process caused by gastric acid, Helicobacter pylori, and/or NSAIDs, resulting in duodenal and/or gastric ulcers. This complete picture highlights the importance of past life experience in peptic ulcers and visualizes the non-causal roles of gastric acid, Helicobacter pylori, and NSAIDs. Significantly, the holistic view provided by the complete picture suggests that life phenomena and diseases are highly complex, and an advanced way of thinking is indispensable for life science and medical studies.
Introduction
Over the centuries, 13 theories have been proposed to explain the pathogenesis of peptic ulcers (including gastric and duodenal ulcers), such as Psychosomatic Theory1,2, Stress Theory3, Nerve Theory4, and ‘No Acid, No Ulcer’5. Although each of these theories explain a minority of characteristics and observations/phenomena of peptic ulcers, they become inconsistent when applied to elucidate the majority of these6. The isolation of Helicobacter pylori (H. pylori) in 1982 was believed to be a revolutionary discovery in peptic ulcer research7,8, and currently, it is widely believed that peptic ulcers are an infectious disease8,9. The etiological theory of peptic ulcers based on H. pylori infection has been designated as Theory of H. pylori10. However, Theory of H. pylori cannot withstand the challenges from the 15 major characteristics and 81 observations/phenomena of peptic ulcers collected from existing data10. For instance, of all the 81 observations/phenomena of peptic ulcers, 45 are unrelated to the infection of H. pylori, making it impossible to elucidate the pathogenesis of peptic ulcers. Moreover, Theory of H. pylori cannot explain 30 of the 36 observations/phenomena associated with the bacterium itself. Furthermore, this theory cannot identify the roles of gastric acid and NSAIDs in peptic ulcers11–15, and it cannot resolve the mysteries of the birth-cohort phenomenon16,17 and seasonal variations18 of peptic ulcers along with the morphology19,20, predilection sites21, relapse22 and multiplicity23 of gastric ulcers.
To address these challenges, a Complex Causal Relationship (CCR), which might be universally applicable to understand any life phenomenon and human disease24, was proposed in 2012. This causal relationship dictates that all life phenomena and human diseases are driven by the invisible, intangible, and incorporeal abstract essence of the human body and thus, the early phase of any disease is an abstract process25. When this concept was employed to analyze the existing data, peptic ulcers are identified as a psychosomatic disease triggered by psychological stress, whereas all the concrete aggressive factors in the stomach, gastric acid, H. pylori, and NSAIDs, play a role in only the late phase of peptic ulcerations. Nevertheless, these 3 local factors can cause the early onset of the disease, exacerbate clinical symptoms, delay the healing process, and increase morbidity/mortality rates25,26. The theory based on this new etiology was designated as Theory of Nodes, which addresses all the major characteristics, observations/phenomena, controversies, and mysteries of peptic ulcers in a series of 6 articles (Supplementary Table S1). In the first two articles recently published, 14 major characteristics and 64 observations/phenomena of peptic ulcers have been explicitly elucidated (Supplementary Table S2-S6), most of which have never been fully understood before. This third article will further discuss the etiology of peptic ulcers, and combine the pathological processes described in the first two articles together to paint a complete picture of the pathogenesis of peptic ulcers. The holistic view allows us to obtain an in-depth and comprehensive understanding of the etiology of peptic ulcers, as well as the roles of gastric acid, H. pylori, and NSAIDs in the disease, thereby providing valuable references for clinical diagnosis, etiological treatments, and evaluating prognosis.
Methods
Five steps were taken to achieve the goal of this study. First, the issues in the etiological concept of modern peptic ulcer research were examined. Second, historical data supporting Stress Theory was briefly reviewed and this theory was used to explain several epidemiological observations. Third, two new concepts, life-view and historical perspective, were introduced to elucidate the early phase of peptic ulcers. Fourth, a summary of the etiology discussed herein and the pathological processes described in the first two articles of the series painted a complete picture of the pathogenesis of peptic ulcers. Fifth, the holistic approach elucidated a consistent pattern of factors to predict which individuals would have peptic ulcers, and proposed a complete cure of the disease without relapse.
Results
The Traditional Etiological Concept in Modern Peptic Ulcer Research
The traditional etiological concept of modern medicine believes that peptic ulcers are caused by the imbalance of defensive and aggressive factors in the upper gastrointestinal tract27,28. As a result, peptic ulcers are considered a local disease by default and modern medical doctors focus their eyes only on the local gastroduodenal mucosa while looking for etiological factors. Consequently, the local aggressive factors, gastric acid, H. pylori, and NSAIDs, were proposed one after another to be the cause of peptic ulcers. However, diabetes patients may become blind and the pathological lesion is in the eyes, but the vision loss is a result of lower secretion of insulin from the pancreas; the pathological lesions of cardiomegaly are in the heart, but these are correlated with the chronic disturbance of pulmonary circulation in the lungs. The mechanisms of both diseases suggest that the origins of disease and the pathological changes could present in different organs. Therefore, the traditional etiological concept is insufficient to discover the cause of the disease, and peptic ulcers may not be a local disease but a general disease due to the abnormalities in other parts of the human body.
Peptic Ulcerations are Triggered by Psychological Stress
After Hans Selye proposed Stress Theory in 19503, much work has been done to substantiate the causal relationship between psychological stress and peptic ulcers. In 1951, Gary proposed that emotional stress and anxiety induce gastrointestinal ulceration by a hormonal mechanism through the hypothalamic-pituitary-adrenal-gastric axis29. In 1983, Peters and Richardson summarized previous studies and their own observations, concluding that stressful life events frequently precede the onset of ulcer symptoms in both newly diagnosed and chronic ulcer patients30. Numerous epidemiological observations suggested a causal relationship between psychological stress and peptic ulcers. Doll and Jones’ survey in 1951 suggested a positive correlation between stressful occupations and duodenal ulcers, a decreased incidence of ulcers among agricultural workers due to the simplicity of their lives, and a greater frequency of gastric ulcers among individuals of poor economic status31. In a birth-cohort study in 1962, Susser and Stein speculated that the English cohorts born in the last quarter of the 19th century were the chief victims of World War I and the economic crisis of the 1930s, thereby experiencing an especially stressful life, leading to higher incidences of peptic ulcers17.
Unfortunately, the causal relationship to identify the etiology of disease and the methodologies essential for data analyses have never been established in modern medicine. As a result, the roles of psychological stress in peptic ulcers remain uncertain, and Stress Theory alone can not explain the major characteristics and observations/phenomena of peptic ulcers, even though it was supported by both medical professionals and lay public33. Consequently, Stress Theory were discredited soon after H. pylori was isolated in 19829, resulting in many unexplained epidemiological observations. In contrast, Theory of Nodes considered psychological stress a trigger of peptic ulcerations and therefore, many epidemiological observations, which previously remained mysterious, can now be elucidated. For example, the continuous decrease of peptic ulcers in 1970-1978 in the US33 can be explained by the improvement of living conditions, better protected human rights, and labour and social security. This explanation is also applicable to the decrease of hospital admissions in England, Wales, and Scotland from 1958-197234, and the data recorded by Scottish Health Services from 1968 to 197535. Moreover, the admissions for peptic ulcers in Hong Kong from 1970 to 1980 increased by 21%, perforations increased by 71%, and the percentage of men over 60 with perforation rose from 18.1 to 24.436. Koo speculated that the serious social strains caused by unexpected population increase and the lowered living standard due to a large number of new immigrants accounted for the increases36. Hui and Lam’s semi-quantitative analysis of negative social events from 1962 to 1985 in Hong Kong also discovered a direct relationship between peptic ulcer and stress on a community scale37. All these suggest that the increase and decrease of peptic ulcers in the populations can be elucidated by Stress Theory.
Before 1900, gastric ulcers were more prevalent than duodenal ulcers and they occurred in more women than men. In the 1900s, the ratios of gastric ulcer: duodenal ulcer and women: men have reversed whereby the incidences of duodenal ulcers declined with a greater prevalence of gastric ulcers and occurring more with men than women. Data indicates the sex ratio, from 3 females: 1 male to 4 males: 1 female for gastric ulcers and 10 males: 1 female for duodenal ulcers while the gastric ulcer: duodenal ulcer ratio from 4 gastric ulcers: 1 duodenal ulcer in 1900 increased to about 10 duodenal ulcers: 1 gastric ulcer in the 1960s20. In Theory of Nodes, these reversals are due to the profound changes in social environments during the 20th century. The reversal of the sex ratio can be explained by the liberation and improved social status for women. The civilization and urbanization, etc. resulted in the reversal of the gastric ulcer: duodenal ulcer ratio. Before 1900, threats to life or survival-related challenges and the severe shortages of supplies for the populace determined the majority of peptic ulcer cases were gastric ulcer patients. However, after 1900, especially after World War II, most of the threats to survival disappeared and the steady growth of people's living standard led to the decreased incidence of gastric ulcers, whereas the fast rhythm of modern life, fierce social competition, and unhealthy lifestyles, etc., primarily induce duodenal ulcers. Therefore, changes in lifestyle after World War II caused the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach of more people in the population, resulting in the reversal of the gastric ulcer: duodenal ratio. These reversals implicate that peptic ulcers are not an infectious disease, but a typical psychosocial disease32,38.
Notably, Theory of Nodes elucidated that there are two sources of stress that may trigger peptic ulcers. Exogenous stress is induced by external factors that give rise to a negative feeling or cause exhaustion, such as negative life events, tense family relationships, stressful environments or occupations. Endogenous stress is induced by internal factors coming from the inner conflicts, such as personality traits, dependency, loneliness, personal threat and goal frustration39, making the individual stressful from time to time. Therefore, the routine method, surveys by questionnaire40, which primarily investigate the psychological stress derived from life events, cannot be used to prove a causal relationship between psychological stress and peptic ulcers32.
Peptic Ulcers are a Typical Psychosomatic Disease
Although Stress Theory is essential to understand the pathogenesis of peptic ulcers, this theory alone is insufficient to explain why the whole population in the same country/region experience the same stressful social events, but only 10~30% of people suffer from peptic ulcers32. Theory of Nodes dictates that Psychosomatic Theory is indispensable to understand the early phase of peptic ulcers. Psychosomatic factors act on the human body for a long time, causing the hyperplasia and hypertrophy of gastrin and parietal cells or a negative life-view in the early phase. However, psychosomatic factors cannot cause peptic ulcers unless there is a trigger, psychological stress. The hyperplasia and hypertrophy and/or negative life-view potentiate the individual’s response to immediate psychological stress, resulting in duodenal and gastric ulcerations, respectively. For this reason, both psychosomatic factors and psychological stress are essential to induce peptic ulcerations and therefore, Psychosomatic Theory and Stress Theory were integrated into a complete etiological theory of peptic ulcers in Theory of Nodes.
An investigation of individual cases within a population helps to understand the roles of psychosomatic factors in peptic ulcers. A general view or attitude about life and environment determined whether an individual would be influenced by the immediate social or natural events. For example, peptic ulcers in children are a rare disease as compared to adults41,42. The rarity of peptic ulcers in childhood can be explained by the fact that most children do not comprehend the gravity of life events or how the events affect them in the future. Major life events and psychological distress during childhood and adolescence might differ in some fundamental ways from adulthood43. Children are comfortable in their own skin and not as effected by social expectations. For example, very young children appear to be less distressed than adults experiencing similar levels of deprivation44,45. Their different feelings and mindset, as compared to adults, suggest they experience less stress44,45, resulting in the rarity of peptic ulcers in children.
Additionally, adults experiencing the same crucial events may not be impacted in the same way. For example, some adults may believe that they can benefit from a global crisis such as war, or they may perceive the loss of a family member as beneficial for their personal social or financial state. Another typical example is that being imprisoned may cause stress in most people, but others may regard the prison as a shelter or opportunity for health care. A survey showed nearly 30% of homeless people intentionally commit minor crimes, such as shoplifting, in the hopes of being taken into custody for the night46. During a television interview with FOX31 Denver News, a prisoner said ‘all what I did was to commit misdemeanor crimes to get in here to get help (medical care and housing)’47. The evidence above suggests that view/attitude towards the same life events varies between individuals, partially explaining why the whole population experience the same stressful social events, but only a small proportion of people suffer from peptic ulcers.
The Concepts of ‘Life-view’ and ‘Historical Perspective
For an in-depth understanding of the etiology of peptic ulcers, we explore why viewpoints or attitudes towards the same life event vary amongst individuals. In fact, before a life event occurs, an individual has already had a general view or attitude about herself/himself, past and future life, the world, and human society. This view or attitude determines the individual’s psychological reaction to the current life event, which is reflected by her/his behaviour and conduct, such as the choices she/he will make, how much effort she/he will spend, how she/he will handle the challenges she/he is facing, and the degree of anxiety or confidence she/he will possess. For ease of reference, lifeâview is defined as the pre-existing, generalized viewpoint or attitude that determines an individual’s behaviour and reaction to life events. If an individual’s life-view is positive and optimistic, her/his reactions to current life events are more likely to be constructive and favourable. As a result, this individual will be less susceptible to life event induced stress. In contrast, if an individual’s life-view is negative and pessimistic, her/his reaction to current life events might be negative and pessimistic. Consequently, she/he is more likely to be influenced by life events and suffer stress, and this individual in more likely to become an ulcer patient. A multi-dimensional case-controlled study discovered that ‘ulcer patients exhibited significantly more emotional distress in the form of depression and anxiety’48. This result supports the roles of life-view in the pathogenesis of peptic ulcers. Maxwell Maltz described a concept of ‘self-image’, which is very similar to life-view proposed herein. He believed that self-image was ‘the cornerstone of all the changes that take place in a person; if one's self-image is unhealthy or faulty — all of his or her efforts will end in failure’49.
Notably, life-view varies individually and therefore, how individuals react to the same life event is individually different. An individual’s life-views are determined by kaleidoscopic past life experiences. Maxwell Maltz believed that ‘self-image is changed, for better or worse, not by intellect alone, or by intellectual knowledge alone, but by 'experiencing'; wittingly or unwittingly, you developed your self-image by your creative experiencing in the past’49. Therefore, life-views are influenced by all the life events, trivial or crucial, experienced by the individuals, and an individual’s life-view evolves every day, especially influenced by home environment, education level, work history, social circle, romantic relationships27. As a result, individuals in the same region react diversely despite experiencing the same life events. Some may experience higher levels of stress while others experience very little stress. It is very likely that only ‘high stress level’ individuals become peptic ulcer patients, further explaining why the population on a whole experience the same stressful life events, but only a small proportion (10-30%) of individuals have peptic ulcers32.
The CCR dictates that different parts of the human body, and/or its surrounding environments, social or natural, are universally inter-correlated not only in space as indicated in integral perspective, but also in time. Thus, another new concept, historical perspective, was deduced to understand the etiology of human disease. This concept suggests that although a life event has passed, its impacts will continue over time, affecting the individual by means of memory, life experience, and/or life-view. Past life experiences contribute to individuals’ life-views as a whole, influencing how they react to the current life event. In Theory of Nodes, life-view dictates whether current life events can trigger psychological stress and thus, is a cornerstone for the development of peptic ulcers. For this reason, while we are investigating the cause of peptic ulcers, the historical events the patient experienced should be taken into consideration, indicating life-view is the core of psychosomatic factors, which represents not a single factor, but the accumulated effects of multiple psychological factors experienced by the individual over a lifetime. Unequivocally, it is life-view that determines the consequence of current life events, ultimately resulting in peptic ulcers and/or other diseases.
Historical perspective was previously defined as ‘the study of a subject in light of its earliest phases and subsequent evolution’50. Notably, Historical perspective is one of the core ideas of German Classical Philosophy51. Herein, historical perspective was proposed to be the concept that historical life events influence or determine the present psychological status, behaviour and attitude towards life of an individual. Another similar concept is historical knowledge, which is the perpetuation of past acts in the present52, suggesting that only after we have known an individual’s past life experiences, can the current psychological reactions and behaviours be fully understood. Although ‘retrospective medical history’ is common practice in modern medical clinics, a clear concept of historical perspective has never come into being in life science and medicine. Consequently, the etiologies of many diseases, including peptic ulcers, have yet to be understood53, even though they have been proposed and were supported by strong evidence.
A Bird’s Eye View of the Pathogenesis of Peptic Ulcers
A summary of the analyses above and the first two articles of the series can paint a complete picture of the pathogenesis of peptic ulcers, including the early, intermediate, and late phases of the disease (Figure 1). This picture provides a bird’s eye view of the entire pathological process of peptic ulceration, which visually and directly points out the roles of psychosomatic factors and psychological stress, as well as the roles of H. pylori, gastric acid, and NSAIDs in the disease. It is worth mentioning that this picture was originally achieved from an integration of 5 major etiological theories in history. In Theory of Nodes, due to heredity predispositions, only a proportion of individuals in the population is susceptible to peptic ulcers, and duodenal and gastric ulcer patients belong to two genetically different populations, reflecting the intrinsic material basis of human disease (Fig.1A).
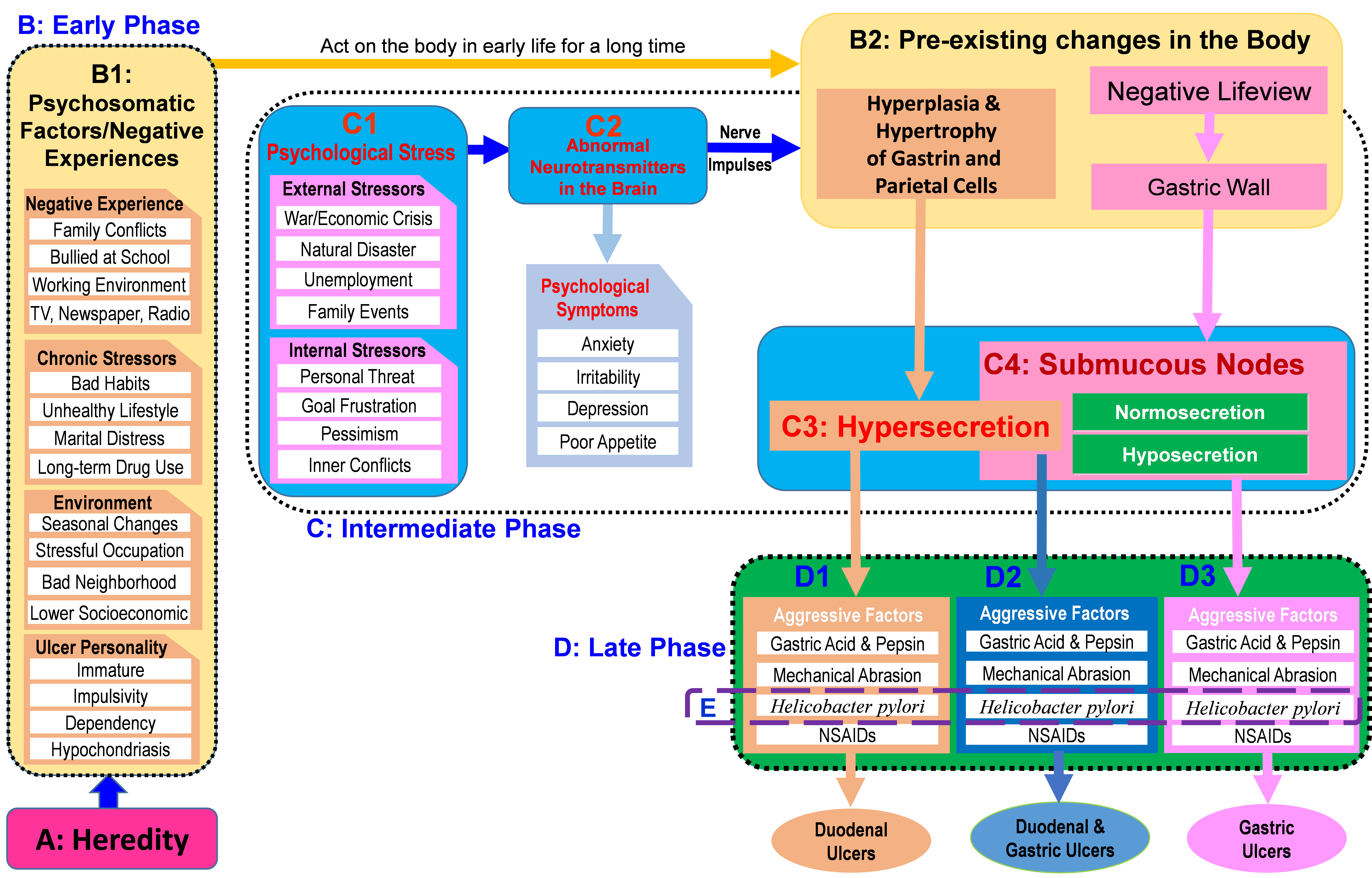
Figure 1: Painting a complete picture of the pathogenesis of peptic ulcers
A. Due to heredity, the individual may have an ulcer personality and thus is susceptible to peptic ulcers. B. The early phase is a long-term abstract psychopathological process, but does not manifest as disease. B1: Multiple psychosomatic factors act on the human body via superposition mechanism. B2: Psychosomatic factors act on the human body for a long time, resulting in the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach and/or a negative life-view. C. The intermediate phase is a short-term process characterized by stress-triggered hypersecretion of gastric acid and/or formation of submucous nodes in the gastric wall. C1: External and internal stressors induce psychological stress. C2: Psychological stress triggers abnormal releases of neurotransmitters in the central nervous system, causing psychological symptoms such as anxiety and poor appetite. C3: Abnormal neurotransmitters cause pathogenic nerve impulses transmitted to the gastric gland, resulting in hypersecretion of gastric acid due to the pre-existing hyperplasia and hypertrophy of gastrin and parietal cells. C4: Abnormal neurotransmitters cause pathogenic nerve impulses transmitted to the stomach, resulting in the formation of submucous nodes in the gastric wall. D. The late phase is a corrosion process caused by local aggressive factors such as gastric acid, H. pylori, and NSAIDs. D1: If only the hypersecretion of gastric acid is induced, the patient has duodenal ulcer. D2: If both the hypersecretion of gastric acid and the formation of submucous nodes are induced, the patient has duodenal and gastric ulcers simultaneously. D3: If only the submucous node is induced, the patient has gastric ulcer, regardless of the normosecretion or hyposecretion of gastric acid. E. H. pylori infection is not essential in many ulcer patients, but a risk factor playing a secondary role in only the late phase of peptic ulcerations.
The early phase starts early in life and is a long-term psychopathological process, but does not manifest as disease (Fig.1B). Multiple psychosomatic factors act on the human body for a long time via superposition mechanism (Fig.1B1), resulting in the hyperplasia and hypertrophy of gastrin and parietal cells in the stomach25, and/or a negative life-view26 (Fig.1B2). Notably, the early phase is an integral and historical process that is invisible, intangible, and incorporeal with very subtle structural and functional changes day by day. The subtle abnormalities in the brain are hard to describe using molecular tools available in modern medicine. Thus, the early phase is an abstract phase and the longest period in the whole pathological process of peptic ulcers, but has rarely been touched upon by modern medicine.
The intermediate phase starts from the perception of psychological stress and ends with the hypersecretion of gastric acid and/or the formation of submucous nodes (Fig.1C). Psychological stress can be induced by either external or internal stressors, or both (Fig.1C1), causing abnormal neurotransmitter release in the central nervous system and therefore, peptic ulcers are usually accompanied by psychological symptoms (Fig.1C2). The abnormal neurotransmitter releases cause the hypersecretion of gastric acid due to the pre-existing hyperplasia and hypertrophy of gastrin and parietal cells (Fig.1C3), or the formation of submucous nodes in the gastric wall due to the negative life-view (Fig.1C4). Thus, the intermediate phase is an effector phase with visible, tangible and corporeal structural and/or functional changes. Notably, the hypersecretion of gastric acid and/or the formation of submucous nodes in the intermediate phase are induced by only the pathogenic nerve impulses from the central nervous system, and do not involve any of the local aggressive factors in the stomach.
The late phase of peptic ulceration is a corrosion process caused by the local aggressive factors (Fig.1D). If only the hypersecretion of gastric acid is induced in the intermediate phase, and the total sum of intensities from all the local aggressive factors surpasses the tolerance threshold, the individual will suffer duodenal ulcer (Fig.1D1). If both the hypersecretion of gastric acid and the formation of submucosal nodes were induced, the individual may suffer duodenal and gastric ulcers simultaneously (Fig.1D2). If only the formation of submucosal nodes were induced, the individual will suffer gastric ulcers (Fig.1D3). Unequivocally, H. pylori plays a role in only the late phase of peptic ulcerations (Fig.1E), further indicating it is not a cause/an etiological factor of peptic ulcers, but a risk factor causing early onset, exacerbating symptoms, delaying the healing process, and increasing morbidity and mortality rates of the disease.
Factors that Predict the Occurrence of Peptic Ulcers
Walsh and Peterson concluded that ‘no consistent pattern of factors, in either host or organism, has been identified that successfully predicts which infected persons will subsequently have ulcer disease’ in 199553. Since then, little progress has been made and thus, Walsh and Peterson’s statement continues to influence current peptic ulcer research. According to the complete picture painted above, the occurrence of peptic ulcers is predictable if the following 4 preconditions are satisfied.
Heredity predisposition for peptic ulcers
In Fig.1A, Theory of Nodes emphasizes that heredity is an innate factor playing a baseline role in peptic ulcers, which predisposes a proportion of individuals in the population to an ulcer personality48. Gastric ulcer patients have a genetic background for gastric ulcers, whereas duodenal ulcer patients have a genetic predisposition for duodenal ulcers. Notably, it is very likely that an individual has a genetic background for both gastric and duodenal ulcers, potentially leading to both types of ulcers simultaneously. Existing data suggests that only ~7% duodenal ulcer patients concomitantly suffer from gastric ulcers54,55. Thus, while the hypersecretion of gastric acid causes duodenal ulcers, it cannot lead to gastric ulcers in the majority (93%) of duodenal ulcer patients, further suggesting that the hypersecretion of gastric acid is not the cause of gastric ulcers.
Hyperplasia and hypertrophy in the stomach and/or a negative life-view
Not all the members in a family suffer from peptic ulcers despite sharing the same genetic background, indicating non-genetic factors are also involved in the occurrence of this disease20,56. In Theory of Nodes, various psychosomatic/environmental factors gradually transformed into pathological changes in the human body (Fig.1B1), the hyperplasia and hypertrophy of gastrin and parietal cells and/or a negative life-view (Fig.1B2). This transformation occurs in the early phase but does not manifest as any disease. Nevertheless, it potentiates the individual’s response to immediate psychological stress, eventually resulting in duodenal and/or gastric ulcers. From the 1900’s to the 1950’s, men were often the direct participants of various social conflicts such as wars and financial crisis, and they were more likely to bear economical pressures than women, thereby explaining the autopsy findings that a higher percentage of males (20-29%) have suffered from ulcers in the past or at present than females (11-18%) in autopsy reports57–59. Thus, the abstract ‘early phase’ is the cornerstone for a full understanding of all the clinical, epidemiological, and laboratory observations of peptic ulcers, highlighting the pivotal role of psychosomatic factors/past life experiences in the disease.
Psychological stress is essential to trigger peptic ulceration
In Theory of Nodes, in addition to hereditary predisposition and psychosomatic factors, psychological stress is a third factor essential to trigger pathogenic nerve impulses to the stomach, eventually resulting in peptic ulcerations. Therefore, it is common to report that stressful life events frequently precede the onset of ulcer symptoms in new and chronic ulcer patients30. Notably, psychological response to life events varies individually, temporally, regionally, and culturally and therefore, an event that is extremely influential for one individual may have no impact on others. It is likely that an individual, who has the genetic background and is affected by psychosomatic factors, does not care about the consequence of a seemingly stressful life event. In that case, no psychological stress was induced and the individual will not suffer peptic ulcers. All these indicate that psychological stress is a subtle mental process, making it challenging to predict who will become stressful after a life event.
H. pylori infection and NSAIDs usage
In Theory of Nodes, without H. pylori infection and NSAIDs usage, the majority of individuals with mild and moderate hyperplasia and hypertrophy of gastrin and parietal cells will not develop duodenal ulcers. Similarly, without H. pylori infection or NSAIDs usage, the individuals impacted by psychological stress may have smaller submucous nodes in the gastric wall with milder symptoms and therefore, they tend to not see a doctor and become subclinical gastric ulcer patients. In contrast, the presence of H. pylori and/or NSAIDs significantly increases the total corrosive intensity in the gastro-duodenum and thus, they interfere the natural courses of both duodenal and gastric ulcers, causing early onsets of the disease, exacerbating clinical symptoms, delaying the healing process, and increase the morbidity/mortality rates. Notably, both H. pylori infection and NSAIDs usage are not etiological factors, but risk factors of peptic ulcers, and neither H. pylori infection nor NSAIDs usage is essential for peptic ulceration, especially for those severely impacted by psychological stress. Nevertheless, H. pylori infection and NSAIDs usage are the fourth factor to predict which individual will become an ulcer patient.
Prevention and Treatment of Peptic Ulcer Disease
Out of all the 4 factors discussed above, heredity is an innate property of the individual and thus cannot be targeted by current technologies. Fortunately, all the other three factors, psychosomatic factors, psychological stress, H pylori infection and NSAIDs usages, are acquired from life experience and environment. Therefore, these 3 factors can be therapeutically targeted. In addition to the stress management proposed in the first two articles of the series, herein 3 strategies were recommended for a complete cure of peptic ulcers without relapse.
Individual level treatment: mind adjustment
A clinical study reported two symptomatic gastric ulcer cases, of which stressful life events preceded the onset of the disease, and ulcer symptoms subsided after the events were resolved30, indicating that a complete cure of peptic ulcers depends on the resolution of life events and/or the resolution of mental health concerns. In the case where there is no resolution to life events, mind adjustment can help ulcer patients solve mental health concerns. Seeking professional psychological help in the form of psychiatrists or therapists is a good way to achieve mind adjustment, which may help ulcer patients unlock their minds and convert their negative views into positive ones. The prognosis of ulcers should include a mental assessment as the treatment would be incomplete without a psychological consultation60.
In Theory of Nodes, the fast pace of modern life, the intensive social competition, or even wars due to social conflicts, inevitably result in negative impacts and pandemic stress in the population, causing high incidences of peptic ulcers in modern society. Thus, peptic ulcers are in fact a social disease that is manifested from past and current social conflicts. “Disease” can be described as dis-ease, a condition when the body and mind are not at ease with each other, where the mind doesn’t “shut off”, causing the physical body to manifest ailments, like peptic ulcers. Achieving and maintaining a peaceful state of mind is imperative to prevent dis-ease, and this can be done by focusing minimally on daily trivialities including personal gains and losses. Expressing and sharing thoughts and feelings by communicating with others is essential in treating mental health issues and altering thought patterns and life perspectives. An epidemiological survey found that peptic ulcer patients and controls differed not in the number of life events they had experienced, but in the way they looked at and responded to negative life events48, indicating a healthy individual needs a healthy mind. Therefore, mind adjustment is essential for a complete cure of peptic ulcers and can effectively prevent the relapse.
Societal level prevention: promoting harmonies of the environments
In Theory of Nodes, as peptic ulcers are a typical psychosomatic disease, growth environments are extremely important in the development of the disease. Domestic and social conflicts during childhood may distort an individual’s life-view, causing mental and/or physical illness during adulthood61. In contrast, a healthy external environment will help to cultivate positive life-views and minimize the occurrence of peptic ulcers. Components of creating a healthy environment include, but do not exclude, harmonious families and neighborhoods, peaceful and relaxed social surroundings, beautiful and comfortable natural environments, and the feeling of safety. Unequivocally, creating a healthy environment is a huge undertaking, and will require governments to lead and participate on all levels by fulfilling their administrative roles and promoting the harmonies of social and natural environments to their citizens. In addition, all countries should coexist peacefully and respect each other, with open, clear, and non-violent communication being the means to settle disputes. These societal level efforts will maximally reduce social competitions, greed, conflicts, and wars for a healthy environment and thus, the morbidity and mortality rates of peptic ulcers will proportionally decrease to the minimal level, or even eventually disappear altogether. All these indicate that despite a long-term and concerted effort, cultivating positive life-views fundamentally prevents peptic ulcers.
Clinical medications and/or surgeries: a temporary solution
In cases where psychological treatments are not available, especially to those living in developing countries having few psychological specialists, medications and/or surgeries can temporarily help ulcer patients. However, Theory of Nodes suggests that all the medications and surgeries, such as anti-secretory drugs for gastric acid or antibiotics for H. pylori, are not etiological treatments, but only turn clinical patients into subclinical ones, causing relapse or even ‘Once an Ulcer, Always an Ulcer’62. Nevertheless, medications mitigate clinical symptoms, accelerate the healing process of peptic ulcers, and significantly reduce the morbidity and mortality rates, especially for patients with severe complications such as bleeding and perforations. Thus, clinical medication/surgeries are still needed at present but should only be considered a temporary solution.
In short, the therapeutics of peptic ulcer disease includes etiological and symptomatic treatments. Promoting social harmony and mind adjustment are essential etiological therapy for a complete cure of peptic ulcers without relapse. Medications and surgeries are symptomatic treatments and therefore, should be considered supplementary therapies that relieve clinical symptoms, reduces severe complications, and decreases the morbidity and mortality rates of peptic ulcers.
Discussion
Despite 13 etiological theories being proposed in history, the pathogenesis of peptic ulcers has never been fully understood. Guided by the CCR with its accompanying methodologies, epistemologies, and way of thinking, Theory of Nodes identified that peptic ulcers are a psychosomatic disease triggered by psychological stress. Out of all the 15 characteristics and 81 observations/phenomena of peptic ulcers, 14 characteristics and 64 observations/phenomena have been elucidated by this etiology in the first two of the series. This third article further elucidates 7 observations/phenomena of peptic ulcers (Supplementary Table S2-S6). A summary of the 3 articles forms a complete picture of the pathogenesis of peptic ulcers, which provides a holistic view to visualize the roles of psychosomatic factors, stress, gastric acid, H. pylori, and NSAIDs in the disease. This picture also clarifies that 4 factors altogether predict which individual may suffer peptic ulcers, and proposed the strategy for a complete cure of peptic ulcers without relapse.
The roles of psychosomatic factors and stress were overlooked in ulcer research
The complete picture indicates that Psychosomatics Theory1,2 and Stress Theory3,63 have proposed the correct cause of peptic ulcers more then 70 years ago. Although stress was originally regarded as the cause of peptic ulcers since 1950, this etiology alone could not fully elucidate the pathogenesis of peptic ulcers, and has been re-considered after the discovery of H. pylori64,65. To understand why the roles of psychosomatic factors and stress have been overlooked in modern ulcer research, guided by historical perspective, Theory of Nodes traced the basic theory of modern medicine back to its historical origin, finding that the rapid development of modern science over the centuries greatly supported materialism. This doctrine states that the concrete matter, which is visible, tangible, and corporeal, is the foundation of nature, life, and the human body. Consequently, ‘structure determines function’ becomes a basic concept in modern medicine and it is widely believed that once the structural abnormality was understood, the pathogenesis of disease could also be fully understood. Currently, this concept is omnipresent in medical studies, and 3 concrete aggressive factors, gastric acid, H. pylori, and NSAIDs, were proposed one after another to be the cause of peptic ulcers. Apparently, committed to materialism, which takes only the concrete essence (structure) of the human body into consideration, modern medicine is not likely to consider the abstract psychosomatics factors and psychological stress as the cause of disease if there are concrete alternatives.
Moreover, also due to the commitment to materialism, modern medicine focuses heavily on the structural abnormalities of the human body. Consequently, the abstract essence of the human body, such as emotion, wisdom, memory, and social relationships, became outside the scope of modern medical doctors. As a result, the methodologies essential to analyze the abstract psychosomatics factors and psychological stress were not well-developed while structural factors become the sole focus of etiological studies. Thus, despite supports from abundant clinical, laboratory, and epidemiological evidence, Psychosomatics Theory and Stress Theory still could not elucidate the pathogenesis of peptic ulcers. For example, Susser and Stein reported a birth-cohort phenomenon in 1962, in which they speculated that stressors like war, unemployment, and financial crises were the etiological factors of this disease. However, without the corresponding analytical methods, neither Psychosomatics Theory nor Stress Theory can explain the birth-cohort phenomenon of peptic ulcer for 60 years, along with many other characteristics and observations/phenomena. Inevitably, both theories were replaced soon after the discovery of H. pylori and NSAIDs uasge64,65. Unequivocally, besides a definite etiology, effective analytical methods are also required for a full understanding of the pathogenesis of peptic ulcers.
Newton and Einstein were successful in physics, because they took both the concrete (structural ‘matter’) and abstract (non-structural ‘force’) essences into their considerations. Therefore, both of the greatest achievements in physics are not due to monism (referencing materialism) as believed by most modern scientists, but due to dualism, which is a combination of materialism and idealism (focusing on the abstract/non-structural essence). In both macro- and micro-physics, it is the abstract essence that drives the changes of the concrete essence. Conceivably, in life science and medicine, it is also the abstract essence of the human body that drives the development of life phenomena and human diseases. Namely, the abstract psychosomatics factors and psychological stress are the real cause of life phenomena and human diseases. Newton and Einstein’s successes in physics implicate that, opposite to the concept ‘structure determines function’, structural abnormalities in the human body are not the cause of disease, but passively driven by its invisible, intangible, and incorporeal abstract essence. This hypothesis guided Theory of Nodes to identify the etiology of peptic ulcers from historical data, thereby addressing all the characteristics, observations/phenomena, controversies, and mysteries of peptic ulcers within a series of 6 articles. The effectiveness showcased suggests that life science and medicine follow the same principles as physics that the abstract essence drives the changes of the concrete essence and therefore, a viable causal relationship for life science and medicine, the CCR, may have been established24.
Implications from the complete picture of the pathogenesis of peptic ulcers
First, an integration of 5 major etiological theories in history brought together a complete picture of the pathogenesis of peptic ulcers25, suggesting that the data accumulated over the centuries is in fact sufficient to fully understand the pathogenesis of peptic ulcers. Unfortunately, as discussed above, a correct cause like psychosomatic factors and stress could not explain the pathogenesis of peptic ulcers. Consequently, much invaluable data accumulated over the centuries was deemed outdated and remain unanalyzed. In contrast, despite more controversies and mysteries, H. pylori infection has garnered a significant amount of attention as an etiological factor in the past 3 - 4 decades. Second, this picture suggests there is a long-term and abstract early phase in peptic ulcers. However, without the CCR and its accompanying methodologies, this concept ‘abstract early phase’ has never come into being in modern research. As a result, despite being reported in details for many decades, the hyperplasia and hypertrophy of the gastrin and parietal cells and the negative life-view, have never been paid enough attention. Third, this complete picture clarified that gastric acid plays a more important role than H. pylori in duodenal ulcers66,67, and H. pylori infection is not essential in many ulcer patients as observed in clinics14,68,69. Apparently, peptic ulcers are not initiated by abnormal neuro-transmitters, gastric acid, H. pylori, and NSAIDs, but by psychosomatic factors and psychological stress. Thus, Nerve Theory, ‘No Acid, No Ulcer’, and Theory of H. pylori are, in fact not, etiological theories, and all 3 local aggressive factors, gastric acid, H. pylori, and NSAIDs, are not etiological factors, but risk factors playing a role in the late phase of peptic ulcers. Unequivocally, the holistic view provided by the picture highlighted the roles of past life experiences and psychological stress in the occurrence of peptic ulcers.
Historical perspective is an indispensable concept for medical research
The application of new methodological concepts, such as integral perspective25 and historical perspective, distinguished Theory of Nodes from all the other 13 etiological theories originated from modern medicine and thus, the complete picture came into being. Herein, only the importance of historical perspective is discussed. First, since ‘a causal relationship between H. pylori and peptic ulcers’ has led to more controversies and mysteries, guided by historical perspective, Theory of Nodes did not limit its scope on the latest studies on H. pylori, but traced the historical origin of this etiological theory, finding that the traditional etiological concept (peptic ulcers are the result of an imbalance of defensive and aggressive factors in the upper gastrointestinal tract21,70,71’) is questionable. Second, historical perspective guided Theory of Nodes to trace the evolution of etiological studies on peptic ulcers and thus a multidisciplinary view/the complete picture of the disease is obtained. This complete picture suggests that looking at only a narrow snapshot of recent research is insufficient for a complete understanding of the pathogenesis of peptic ulcers, but the historical data accumulated over the centuries proved to be an invaluable resource to reach the goal. Third, historical perspective emphasizes the importance of past life experiences/psychosomatic factors in peptic ulcers, which affect the individual by the hyperplasia and hypertrophy of gastrin and parietal cells or the formation of a negative ‘life-view’. Despite the subtlety, the negative life-view and psychopathological lesions in the early phase are the cornerstones to understanding peptic ulcers; however, both were not recognized in modern medicine. These indicate that the application of historical perspective can help modern medical researchers reach into the immense amount of historical data, allowing them to innovate, create, and apply studies of various life science and medicine as shown in Theory of Nodes.
A new way of thinking is vital for the future development of medicine
The complete picture described herein is relatively more complex than the pictures of the pathogenesis of peptic ulcers illustrated before, suggesting that life phenomena and human diseases are more complicated than modern doctors anticipate. This picture also indicates that life phenomena and human diseases are much more complex than the phenomena in physics. Accordingly, the causal relationship in life science and medicine is much more complex than that in physics and therefore, it is termed Complex Causal Relationship. Unequivocally, due to the high complexity of life and the human body, life scientists and doctors have to take much more into consideration in their research.
In physics, the causal relationship is relatively simple: one and/or a couple of causes versus one and/or a couple of effects. Accordingly, the studies in Newton and Einstein’s days are usually quite straightforward, which only investigate one or a couple of variables, but keep all the others unchanged. This thought process is termed as ‘linear way of thinking’72. In contrast, the causal relationship in life science and medicine is much more complex. The human body can be divided into a structural hierarchy consisting of 8-levels, which does not exist in physical science but include: society, individual, system, organ, tissue, cell, organelle, and biomolecule. At each level, there are many different entities and inter-correlations. As a result, studies in life science and medicine are usually multifactorial, obscure, and twisty, which require multiple variables to be simultaneously investigated. For example, even though peptic ulcers are a relatively simple disease, Theory of Nodes suggests that their causes vary individually, regionally, culturally, and historically, and the effects (pathogenesis) include 15 major characteristics and 81 observations/phenomena. In this case, the linear way of thinking used by Newton and Einstein in physics does not match the high complexity of life science and medicine.
To understand a life phenomenon or human disease, we have to think much more comprehensively than the studies in physics. In life science and medicine, we frequently need to apply multiple concepts to resolve an issue due to their complex nature. In Theory of Nodes, the etiological factors exist in other organs distant from the lesions in the gastro-duodenum, or are life events experienced long time ago. Therefore, when studying life phenomena and human diseases, we should always keep the concepts of integral perspective and historical perspective in mind. Moreover, the causes of life phenomena and human diseases are often ‘multifactorial’. Accordingly, we may have to superpose the effects of multiple individual factors as elucidating the roles of the aggressive factors in peptic ulcers26. Thus, superposition mechanism is a very basic methodology to elucidate many life phenomena or human diseases. Additionally, ‘multifactorial’ also means complex and confusing, indicating we should always keep an eye on illusions in life science and medical studies. Therefore, the high complexity of life science and medicine necessitates us to consider much more, like factors, principles, and concepts, simultaneously as it has been shown in Theory of Nodes, though these are generally not essential in physics. This thought process was termed multi-dimensional way of thinking24, which is one of the keys to a full understanding of peptic ulcers in Theory of Nodes.
In short, the linear way of thinking used in physics no longer matches the needs of life science and medicine. The highly complex life phenomena and human diseases necessitate a conversion from the current way of thinking used in modern medicine to a more advanced multi-dimensional way of thinking, which takes much more into consideration, and analyzes and deals with many problems from multiple angles – all simultaneously. This conversion is vital for life science and medicine in this 21st century.
Conclusions
An integration of 5 etiological theories in history painted a complete picture of the pathogenesis of peptic ulcers, suggesting that the empirical data accumulated over the centuries is sufficient to fully understand the pathogenesis of peptic ulcers. However, the theories and methodologies essential for data analyses have never been established. Multiple psychosomatic factors act on the human body for a long time via superposition mechanism, resulting in the hyperplasia and hypertrophy of gastrin and parietal cells and/or a negative life-view. These pre-existing lesions potentiate the individual’s response to current psychological stress, which triggers the release of neurotransmitters in the central nervous system and the transmission of pathogenic nerve impulses to the stomach, causing hypersecretion of gastric acid and/or submucous nodes in the gastric wall. Finally, the corrosive effects of gastric acid, H. pylori, and NSAIDs lead to all the clinical symptoms. This picture elucidates that 4 factors can predict which individual will have peptic ulcers, and proposed mind adjustment and creating harmonious environments for a complete cure of the disease without relapse. The wide application of historical perspective potentially leads to ground-breaking insights for disease, and a multi-dimensional way of thinking is vital for the future development of life science and medicine.
Acknowledgements
Special thanks to Katelynn J. Rowe, who contributed time and effort to challenge the ideas, optimize the structure, and enrich the contents of the article. I would like to thank Douglas Rowe, Jonathan Weldrick, and Angela Haworth for draft revisions. I would also like to thank Dr. Xiao Xiang and Dr. Stephen Holland for their constructive comments.
Author contribution
SXMD conceived the idea, collected and analyzed data, interpreted the analyses into figures, and drafted the manuscript.
Competing interest statement
The author has no conflict of interest to report.
Data availability statement
All the supporting data in this article are published papers or books, or in the supplementary files.
Supplemental Materials
The supplemental material includes 6 tables as attached.
ORCID: Simon Xin Min Dong: htps://orcid.org/ 0000-0003-0073-7216
References
- Wolowitz HM. Oral involvement in peptic ulcer. J Consult Psychol. 1967;31(4):418–419.
- Alexander F. Fundamental Concepts of Psychosomatic Research: Psychogenesis, Conversion, Specificity. Psychosom Med. 1943 Jul;5(3):205.
- Selye H. The physiology and pathology of exposure to stress. Oxford, England: Acta; 1950.
- Bergmann G von. Ulcus duodeni und vegetatives nerve system. Berl Klin Wchnscher. 1913;50:2374.
- FatoviÄ-FerenÄiÄ S, BaniÄ M. No acid, no ulcer: Dragutin (Carl) Schwarz (1868-1917), the man ahead of his time. Dig Dis. 2011;29(5):507–10.
- Kuang H. Peptic Ulcer Diseases. Beijing: People’s Medical Publishing House; 1990.
- Ciacci C, Mazzacca G. The history of Helicobacter pylori: A reflection on the relationship between the medical community and industry. Dig Liver Dis. 2006 Oct;38(10):778–780.
- Charitos IA, D’Agostino D, Topi S, Bottalico L. 40 Years of Helicobacter pylori: A Revolution in Biomedical Thought. Gastroenterol Insights. 2021 Mar 24;12(2):111–135.
- Zetterström R. The Nobel Prize in 2005 for the discovery of Helicobacter pylori: Implications for child health. Acta Paediatr Int J Paediatr. 2006;95(1):3–5
- Dong SXM, Chang CCY, Rowe KJ. A collection of the etiological theories, characteristics, and observations/phenomena of peptic ulcers in existing data. Data Br. Elsevier Inc.; 2018 Aug;19:1058–1067.
- Go MF, Graham DY. How does Helicobacter pylori cause duodenal ulcer disease: The bug, the host, or both? J Gastroenterol Hepatol. 1994 Jan;9(S1):S8–S12.
- Tovey FI, Hobsley M. Review: is Helicobacter pylori the primary cause of duodenal ulceration? J Gastroenterol Hepatol. 1999 Nov;14(11):1053–1056.
- Yeomans ND. The ulcer sleuths: The search for the cause of peptic ulcers. J Gastroenterol Hepatol. 2011 Jan;26(SUPPL. 1):35–41.
- Gisbert JP, Calvet X. Review article: Helicobacter pylori-negative duodenal ulcer disease. Aliment Pharmacol Ther. 2009 Oct;30(8):791–815.
- Musumba C, Pritchard DM, Pirmohamed M. Review article: cellular and molecular mechanisms of NSAID-induced peptic ulcers. Aliment Pharmacol Ther. 2009 Sep;30(6):517–531.
- Sonnenberg A, Müller H, Pace F. Birth-cohort analysis of peptic ulcer mortality in Europe. J Chronic Dis. 1985 Jan;38(4):309–317.
- Susser M, Stein Z. Civilization and Peptic Ulcer. Lancet. 1962 Jan 20;279(7221):116–119.
- Sonnenberg A, Wasserman IH, Jacobsen SJ. Monthly variation of hospital admission and mortality of peptic ulcer disease: A reappraisal of ulcer periodicity. Gastroenterology. 1992 Oct;103(4):1192–1198.
- Carton J, Daly R, Ramani P. Clinical Pathology. Oxford University Press; 2007.
- Damon A, Polednak AP. Constitution, genetics, and body form in peptic ulcer: A review. J Chronic Dis. 1967 Oct;20(10):787–802.
- Malfertheiner P, Chan FKL, McColl KEL. Peptic ulcer disease. Lancet. 2009;374(9699):1449–1461.
- Parsonnet J. Helicobacter pylori: the size of the problem. Gut. 1998 Jul 1;43(Supplement 1):S6–S9.
- Quan C, Talley NJ. Management of peptic ulcer disease not related to Helicobacter pylori or NSAIDs. Am J Gastroenterol. The American College of Gastroenterology; 2002 Dec;97(12):2950–2961.
- Dong SXM, Chang CCY. Philosophical Principles of Life Science. Wunan Cult. Enterp. Taipei: Wunan Culture Enterprise; 2012.
- Dong SXM. The hyperplasia and hypertrophy of gastrin and parietal cells induced by chronic stress explain the pathogenesis of duodenal ulcer. J Ment Heal Clin Psychol. 2022;6(3):1–12.
- Dong SXM. A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers. J Ment Heal Clin Psychol. 2022;6(3): 13-24.
- Søreide K. Current insight into pathophysiology of gastroduodenal ulcers. J Trauma Acute Care Surg. 2016 Jun;80(6):1045–1048.
- Shay H. Aetiology and pathology of gastric and duodenal ulcer. Gastroenterology. Bockus Gastroenterology, 2nd Edition; 1953;1:420–465.
- Gray SJ, Jr. JAB, Spiro RW, Reifenstein HM. Chronic Stress and Peptic Ulcer: I Effect of Corticotropin (ACTH) and Cortisone on Gastric Secretion. 1951;147(16):1529–1537.
- Peters MN, Richardson CT. Stressful Life Events, Acid Hypersecretion, and Ulcer Disease. Gastroenterology. 1983 Jan;84(1):114–119.
- Doll R, Jones FA, Buckatzsch MM. Occupational Factors in the Aetiology of Gastric and Duodenal Ulcers, with an Estimate of their Incidence in the General Population. Br J Ind Med. London: H. M. Stationery Office; 1951 Oct 1;8(4):308–309.
- Jones MP. The role of psychosocial factors in peptic ulcer disease: Beyond Helicobacter pylori and NSAIDs. J Psychosom Res. 2006;60(4):407–412.
- Elashoff JD, Grossman MI. Trends in Hospital Admissions and Death Rates for Peptic-Ulcer in the United-States from 1970 to 1978. Gastroenterology. 1980;78(2):280–285.
- Brown RC, Langman MJS, Lambert PM. Hospital admissions for peptic ulcer during 1958-72. BMJ. 1976 Jan;1(6000):35–37.
- Jibril JA, Redpath A, Macintyre IMC. Changing pattern of admission and operation for duodenal ulcer in Scotland. Br J Surg. 1994 Jan;81(1):87–89.
- Koo J, Ngan YK, Lam SK. Trends in hospital admission, perforation, and mortality of peptic ulcer in Hong Kong from 1970 to 1980. Gastroenterology. Elsevier Masson SAS; 1983 Jun;84(6):1558–1562.
- Hui WM, Lam SK, Shiu LP, Ng MMT. Semi-quantitative study of negative social events, stress and incidence of perforated peptic ulcer in Hong Kong over 24 years. Gastroenterology. 1990;98:A61.
- Levenstein S. The Very Model of a Modern Etiology: A . Biopsychosocial View of Peptic Ulcer. Psychosom Med. 2000;62(2):176–185.
- Ellard K, Beaurepaire J, Jones M, Piper D, Tennant C. Acute and chronic stress in duodenal ulcer disease. Gastroenterology. 1990 Dec;99(6):1628–1632.
- Kurata JH, Nogawa AN, Abbey DE, Petersen F. A prospective study of risk for peptic ulcer disease in seventh-day adventists. Gastroenterology. 1992 Mar;102(3):902–909.
- Sullivan PB. Peptic ulcer disease in children. Paediatr. Child Health (Oxford). 2010. p. 462–464.
- Guariso G, Gasparetto M. Update on Peptic Ulcers in the Pediatric Age. Ulcers. 2012;2012:1–9.
- Compas BE. Stress and life events during childhood and adolescence. Clin Psychol Rev. 1987;7(3):275–302.
- Rosenberg M, Simmons RG. Black and White Self-esteem: The Urban School Child. Contemp Sociol. 1975 May;4(3):281.
- McLeod JD, Shanahan MJ. Poverty, Parenting, and Children’s Mental Health. Am Sociol Rev. 1993 Jun;58(3):351.
- Ramesh R. A fifth of all homeless people have committed a crime to get off the streets. Guard. 2010.
- Chris Halsne. Expensive trend: People committing crimes to get free jail health care. Fox 31 Denver News 2014.
- Feldman M, Walker P, Green JL, Weingarden K. Life events stress and psychosocial factors in men with peptic ulcer disease: a multidimensional case-controlled study. Gastroenterology. 1986 Dec;91(6):1370–9.
- Maltz M. Psycho-Cybernetics: A New Way to Get More Living out of Life. Prentice-Hall; 1960.
- Lawrence BS. Historical Perspective: Using the Past to Study the Present. Acad Manag Rev. 1984 Apr;9(2):307–312.
- Little D. Philosophy of History [Internet]. Stanford Encycl. Philos. (Summer 2017 Ed. Edward N. Zalta 2017.
- Dilthey W. The Construction of the Historical World in the Human Studies. Dilthey: Selected writings. 1976;238.
- Walsh JH, Peterson WL. The Treatment of Helicobacter pylori Infection in the Management of Peptic Ulcer Disease. Wood AJJ, editor. N Engl J Med. 1995 Oct 12;333(15):984–991.
- Johnson HD. The special significance of concomitant gastric and duodenal ulcers. Lancet. Elsevier; 1955;265(6858):266–270.
- Kameyama J, Sasaki I, Imamura M, Sato T. Selection of operation for concomitant gastric and duodenal ulcers. Jpn J Surg. 1983 Jan;13(1):16–19.
- Harvald B, Hauge M. Heredity factors elucidated by twin studies, in Neel JV (ed): Genetics and the Epidemiology of Chronic Diseases. Genet Epidemiol Chronic Dis. 1965;61–76.
- Lindström CG. Gastric and Duodenal Peptic Ulcer Disease in a Well-Defined Population: A Prospective Necropsy Study in Malmö, Sweden. Scand J Gastroenterol. 1978 Feb 23;13(2):139–143.
- Levij IS, Fuente AADELA. A post-mortem study of gastric and duodenal peptic lesions: Part II Correlations with other pathological conditions. Gut. 1963 Dec 1;4(4):354–359.
- Watkinson G. The Incidence of Chronic Peptic Ulcer Found at Necropsy: A Study of 20,000 Examinations Performed in Leeds in 1930-49 and in England and Scotland in 1956. Gut. 1960 Mar 1;1(1):14–30.
- Bytov MA. Etiology and pathogenesis of peptic ulcer. Eksp Klin Gastroenterol. 2003;(5):5-9,192.
- Fava GA, Cosci F, Sonino N. Current Psychosomatic Practice. Psychother Psychosom. 2017;86(1):13–30.
- Katz P. Once an ulcer, always an ulcer? Am J Gastroenterol. 1994 May;89(5):808–809.
- Szabo S, Tache Y, Somogyi A. The legacy of Hans Selye and the origins of stress research: A retrospective 75 years after his landmark brief “Letter” to the Editor #of Nature. Stress. 2012;15(5):472–478.
- Flaskerud JH. Gastric Ulcers, from Psychosomatic Disease to Infection. Issues Ment Health Nurs. Taylor & Francis; 2020 Nov 1;41(11):1047–1050.
- Overmier JB, Murison R. Restoring psychology’s role in peptic ulcer. Appl Psychol Heal Well-Being. 2013;5(1):5–27.
- Ford AC, Talley NJ. Head to Head: Does Helicobacter pylori really cause duodenal ulcers? Yes. BMJ. 2009 Aug 14;339(aug14 1):b2784.
- Hobsley M, Tovey FI, Bardhan KD, Holton J. Head to Head: Does Helicobacter pylori really cause duodenal ulcers? No. BMJ. 2009 Aug 14;339(aug14 1):b2788–b2788.
- Iijima K, Kanno T, Koike T, Shimosegawa T. Helicobacter pylori-negative, non-steroidal anti-inflammatory drug: Negative idiopathic ulcers in Asia. World J Gastroenterol. 2014;20(3):706.
- Wong GLH, Wong VWS, Chan Y, et al. High Incidence of Mortality and Recurrent Bleeding in Patients With Helicobacter pylori-Negative Idiopathic Bleeding Ulcers. Gastroenterology. AGA Institute American Gastroenterological Association; 2009;137(2):525–531.
- Tarnawski A. Cellular Mechanisms of Gastric Ulcer Healing. The Stomach. Berlin, Heidelberg: Springer Berlin Heidelberg; 1993. p. 177–192.
- Hackelsberger A, Platzer U, Nilius M, et al. Age and Helicobacter pylori decrease gastric mucosal surface hydrophobicity independently. Gut. 1998 Oct;43(4):465–469.
- Teal R. Developing a (Non-linear) Practice of Design Thinking. Int J Art Des Educ. 2010 Oct;29(3):294–302.
Supplementary Materials
Table S1: List of 6 articles to explain all the 15 characteristics and 81 observations/phenomena of peptic ulcers
|
Article |
Title |
|
A1 |
The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers. Published on Journal of Mental Health & Clinical Psychology, 2022, 6(3): 1-12. |
|
A2 |
A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers. Published on Journal of Mental Health & Clinical Psychology, 2022, 6(3): 13-24. |
|
A3* |
Painting a Complete Picture of the Pathogenesis of Peptic Ulcers. |
|
A4 |
Novel Data Analyses Explain the Birth-Cohort Phenomenon of Peptic Ulcers. |
|
A5 |
Novel Data Analyses Explain the Seasonal Variations of Peptic Ulcers. |
|
A6 |
Novel Data Analyses Address the African Enigma and The Controversies Surrounding the Roles of Helicobacter Pylori in Peptic Ulcers. |
Note: 1. A1: Article 1. 2. * This article. 3. The 6 articles altogether explained all of the 15 characteristics and 81 observations/phenomena of peptic ulcers. 4.The order and titles of the final published articles may be modified during the publication process.
Table S2: Index of 14 elucidated characteristics of peptic ulcers
|
Classification |
Characteristics |
Explanation in the Article |
Article, Page, Column & Line # |
|
General (3) |
1) Genetic predisposition |
Individuals who are susceptible to gastric and duodenal ulcers belong to two genetically different populations. Notably, some individuals may have the genetic background for both gastric and duodenal ulcers and thus, they may have both types of ulcers simultaneously. |
Article 2, Page 20, Left Column, Lines 14-24. |
|
2) Etiology |
Peptic ulcers are not an infectious disease caused by the H. pylori infection, but a psychosomatic disease triggered by psychological stress. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
|
3) Epidemiology |
|
|
|
|
Clinical symptoms (6) |
4) Predilection sites |
The gastric antrum and lesser curvature have the most complicated function with the largest ganglions and the greatest density of highly developed nerve plexus, determining that the local tissues at these sites receive stronger and more frequent pathogenic nerve impulses from the CNS. |
Article 2, Page 17, Right Column, Line 17-Page 18, Left Column, Line 6. |
|
5) Morphology |
The shape and size of submucous nodes determine the morphology of gastric ulcers. The nodes have a clear border involving the submucosa and muscular layers, determining gastric ulcers have a sharply circumscribed loss of tissue involving the mucosa, sub-mucosa, and muscular layer. Local aggressive factors in the stomach stimulate and corrode the soft tissues around the lesion, causing contraction, denaturation and necrosis. Accordingly, gastric ulcers display a characteristic ‘punch out’ appearance with clean edges. (Figure 1A-G). |
Article 2, Page 17, Left Column, Line 47-Right Column, Line 30. |
|
|
6) Bleeding |
If large blood vessels are close to the nodes, they may rupture due to the corrosive local aggressive factors, causing bleeding. |
Article 2, Page 18, Left Column, Lines 8-28. |
|
|
7) Perforation |
A small node will not penetrate the serosa and rarely results in perforation and the symptoms are less severe. In contrast, a large node may penetrate the serosa, allowing the gastric wall to be perforated when exposed to local aggressive factors. |
Article 2, Page 18, Left Column, Lines 8-28. |
|
|
8) Relapse |
Clinical patients suffer relapses of peptic ulcers because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
|
9) Multiplicity |
The pathogenic nerve impulses from the CNS may affect the tissues at multiple locations in the stomach simultaneously due to the local nerve distribution, causing the multiplicity of submucous nodes in the gastric wall. Clinically, the disease manifests itself as the characteristic of multiplicity. |
Article 2, Page 18, Right Column, Lines 32-39. |
|
|
Local aggressive factors (3) |
10) Gastric acid |
The hypersecretion of gastric acid is an intermediate process of duodenal ulceration, suggesting it is not a cause of duodenal ulcers, but an effect of stress triggered by personality traits or life events. Nevertheless, the hypersecretion of gastric acid is a determinant factor in the late phase of duodenal ulceration, governing many characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-35. |
|
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Gastric acid plays a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 19, Left Column, Lines 2-16. |
||
|
11) H. pylori |
H. pylori infection is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left Column, Line 17; Article 1, Page 7, Right Column, Lines 34-41. |
|
|
H. pylori plays a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 19, Left Column, Line 18-Right Column, Line 12. |
||
|
12) NSAIDs |
NSAIDs usage is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left Column, Line 17; Article 1, Right Column, Page 7, Lines 34-41. |
|
|
NSAIDs are not an etiological factor of peptic ulcers in Theory of Nodes, but a risk factor playing a secondary role in only the late phase of peptic ulcers, exacerbating the clinical symptoms and increasing the clinical morbidity/mortality rates. |
Article 2, Page 19, Right Column, Lines 14-30. |
||
|
Prognosis (3) |
13) Self-healing |
In most cases, especially in those subclinical patients, ulcers heal up automatically due to the resolution of life events. Unfortunately, the local aggressive factors in the stomach, such as gastric acid and pepsin, the infection of H. pylori, NSAIDs, and mechanical abrasions may delay the healing process. |
Article 2, Page 18, Left Column, Lines 30-49. |
|
14) Effects of clinical treatments |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, but the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori-negative Cases D and F, or in the H. pylori-positive Cases J and R. Cases like Cases D, F, J and R explains a dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
|
Medications may attenuate the impact of local aggressive factors, such as inhibiting the hyper-secretion of gastric acid, eradicating H. pylori, increasing the resistance of the mucosa, or protecting the injured mucosa. Thus, medications may be conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 18, Left Column, Lines 42-49. |
||
|
15) Hospitalization rates, morbidity, and mortality
|
Neither H. pylori infection nor NSAIDs usage is an etiological factor. Both play a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symptoms and increasing clinical morbidity and mortality rates. |
Article 1, Page 7, Right Column, Lines34-41.
|
|
|
Gastric acid, H. pylori, and NSAIDs play a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 18, Right Column, Lines 42-52. |
Note: The blank will be filled in other articles of the series
Table S3: Index of 6 elucidated duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
1. No Acid, No Ulcer (True statement for duodenal ulcer). |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDS. |
Article 1, Page 5, Right Column, Lines 28-34. |
|
2. The role of gastric acid in the pathogenesis of duodenal ulcer is further supported by the relief of pain observed after neutralization or buffering of gastric contents with alkali or food. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors. Thus, neutralization or buffering of gastric contents with alkali or food results in the relief of pain in duodenal ulcer patients. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
3. Doll and Jones’ survey suggested a positive correlation between stressful occupations and duodenal ulcer, a decreased incidence of ulcer among agricultural workers. |
Psychosomatic factors such as hypochondriasis, a negative perception of life events, dependency, and lowered self-confidence, made ulcer patients more susceptible to stress than controls. |
Article 1, Page 3, Right Column, Line 36-Page 4, Left Column, Line 9. |
|
4. Studies suggest that severe anxiety caused acid hypersecretion which, in turn, contributed to ulceration and symptoms. The fact that acid hypersecretion and symptoms abated with alleviation of stress supports this hypothesis. |
The hypersecretion of gastric acid is triggered by the perception of stress via vagus nerves, and the hyperplasia and hypertrophy of gastrin and parietal cells in the early phase significantly potentiated the individual’s response to life events. |
Article 1, Page 5, Left Column, Lines 37-43. |
|
5. Rates of recurrence in patients whose initial ulcers healed during conventional anti-secretory therapy range from 60 to 100 percent per year. |
Neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
6. Duodenal ulcer had higher incidence in large cities compared to rural areas in Africa since the 1950’s. |
Life in large cities is more competitive and stressful than in rural areas. |
Article 1, Page 4, Left Column, Lines 9-12. |
Table S4: Index of 9 elucidated gastric ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
7. No Acid, No Ulcer (wrong statements for gastric ulcers). |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
8. In contrast to patients with duodenal ulcer, most patients with gastric ulcer are normo-secretors or hypo-secretors. Decreased acid-peptic activity in these patients suggests impaired mucosal defence. |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid, and it is the pre-existed submucous nodes that account for the impaired mucosal defence. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
9. Gastric ulcer is a sharply circumscribed loss of tissue involving the mucosa, submucosa, and muscular layer and a characteristic “punch out” appearance with clean edges, as if it were cut by a knife. |
The shape and size of submucous nodes determine the morphology of gastric ulcers. The nodes have a clear border involving the submucosa and muscular layers. As a result, gastric ulcers have a sharply circumscribed loss of tissue involving the mucosa, sub-mucosa, and muscular layer. Local aggressive factors in the stomach stimulate and corrode the soft tissues around the lesion, causing contraction, denaturation and necrosis. Accordingly, gastric ulcers display a characteristic ‘punch out’ appearance with clean edges, as if it were cut by a knife. |
Article 2, Page 17, Right Column, Lines 19-30. |
|
10. Gastric ulcers can be induced only in 8-30% of mouse models. |
In addition, gastric ulcer can be induced only in specially bred rat strains, reflecting the impacts of heredity on the occurrence of the disease. In Theory of Nodes, heredity determines that gastric ulcers can be induced only in 8-30% of mouse models. |
Article 2, Page 20, Left Column, Lines 14-27. |
|
11. Gastric ulceration begin in the mucosa and extend into the wall of the stomach. |
Wrong statement. Gastric ulcers are not penetrating lesions beginning in the mucosa and extending into the wall of the stomach, but are ‘primed’ by the necrotic tissues (nodes) pre-existing within the gastric wall, which make the mucosa highly susceptible to the local aggressive factors. |
Article 2, Page 18, Left Column, Lines 19-28. |
|
12. Stress-related gastric lesions are ‘brain-driven’ events that may be more effectively managed through central manipulations than by altering local, gastric factors. For example, stimulation or lesions of the central nucleus of the amygdala produced or reduced gastric ulcers, respectively. |
The consequence of psychological stress in gastric ulcers is the abnormal release of neurotransmitters in the CNS, leading to the transmission of pathogenic nerve impulses to the stomach. Notably, in Theory of Nodes, what Nerve theory discovers is the intermediate phase of peptic ulcerations (Please refer to A1). |
Article 2, Page 16, Left Column, Line 23-Right Column, Line 18. |
|
13. Development of gastric ulcers elicited by cold stress was significantly decreased by i.p. pre-treatment with EDTA or a-methyl tyrosine, which depleted neurotransmitters. Gastric ulcers were significantly increased by pre-treatment with CaCl2. |
The consequence of psychological stress in gastric ulcers is the abnormal release of neurotransmitters in the CNS, leading to the transmission of pathogenic nerve impulses to the stomach. EDTA is a sequestering agent for removing a neurotransmitter, Ca2+; α-methyl tyrosine is a competitive inhibitor for tyrosine in the production of noradrenaline and dopamine. Pre-treating animals with EDTA or α-methyl tyrosine-controlled stress-induced gastric ulcers by reducing neurotransmissions. |
Article 2, Page 16, Left Column, Line 23-Right Column, Line 18. |
|
14. The predilection sites of gastric ulcers are gastric antrum and lesser curvature. |
The gastric antrum and lesser curvature have the most complicated function with the largest ganglions and the greatest density of highly developed nerve plexus. Thus, the gastric antrum and lesser curvature are the predilection sites of gastric ulcers. |
Article 2, Page 17, Right Column, Line 41-Page 18, Left Column, Line 6. |
|
15. Vulnerability to gastric ulceration is modulated by psychologically meaningful experiences. Repeated stress of the same type generally, but not exclusively, provides some degree of protection against ulcer during the second or later exposures. |
Peptic ulcer is a psychosomatic disease triggered by psychological stress, indicating that the perception of stress determines if life events cause ulcer diseases. After repeated exposure to the same stressful life events, the individual may be mentally prepared and respond calmly without the perception of stress. Thus, psychologically meaningful experiences can modulate the vulnerability to gastric ulcers and provides some degree of protection against ulcer during the second or later exposures. |
Article 2, Page 18, Right Column, Lines 22-39. |
Table S5: Index of 26 elucidated both gastric and duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
16. The pathogenesis of NSAID-induced peptic ulcers is complex and multi-factorial. |
A statement based on a wrong etiology. Since NSAIDs usage is not an etiological factor of peptic ulcers, the etiology based on NSAIDs has inevitably led to controversies and challenges in the field, and the classification of peptic ulcers based on H. pylori and NSAIDs does not help to elucidate the pathogenesis of peptic ulcers, but make the pathogenesis of NSAIDs-induced peptic ulcers ‘complex’ or ‘multi-factorial’. |
Article 2, Page 19, Right column, Lines 45-51. |
|
17. 14% of patients taking NSAIDs chronically can be found to have lesions described as gastric ulcers and 10% have lesions describes as duodenal ulcers. |
In duodenal ulcer, it is the hyper-secretions of gastric acid that determines if NSAIDs usage induces duodenal ulcerations, whereas in gastric ulcer it is the pre-existed submucous nodes that determine if NSAIDs usage induces gastric ulcerations. Only the NSAIDs users with the hypersecretion of gastric ulcers or the pre-existed submucous nodes can become duodenal or gastric ulcer patients. |
Article 2, Page 19, Right Column, Lines 14-30. |
|
18. Birth-cohort Phenomenon: the mortality rate of gastric ulcers in England and Wales increased at the beginning of the 20th century, reached a peak and then began to fall in the early 1950s. They also found similar trends for duodenal ulcers but followed approximately five years behind. |
|
|
|
19. Once an ulcer, always an ulcer. |
Clinical patients suffer relapses of peptic ulcers because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
20. Seasonal occurrence of peptic ulcer diseases. |
|
|
|
21. Patients free of ulcer distress for long periods of time were subjected to emotional trauma and feelings of insecurity during the symptom-free intervals. |
For individuals with specific personality traits, even trivialities may cause severe impacts and they are more susceptible to life events. Some patients not subject to crucial life events may still suffer gastric ulceration due to personality traits that cause emotional trauma and feelings of insecurity. Long-term effects from past crucial events and specific personality traits explain the relapse of some individuals without suffering immediate crucial events. |
Article 2, Page 18, Right Column, Lines 10-15. |
|
22. Investigations of the effects of perceived stress on physiological parameters are scarce and the findings are often conflicting. |
Questionnaire-based epidemiological surveys may have discounted many chronic stressors during peptic ulcer research, and that the essential methodology to study psychosocial factors (the abstract essence of the human body) have not been established in modern medicine. |
Article 1, Page 5, Left Column, Line 44-Page 6, Right Column, Line 13. |
|
23. There is no definitive study proving a causal relationship between psychological stress and the development of ulcer disease. |
1. Without the CCR, there is no benchmark to identify the cause of ulcer disease. 2. without the methodological concepts derived from the CCR, much invaluable historical data is deemed outdated and remains unanalyzed. |
Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
24. Feldman’s multidimensional case-controlled study found that ulcer patients exhibited significantly more emotional distress in the form of depression and anxiety. Hypochondriasis, a negative perception of their life events, dependency, and lowered self-confidence were the four variables that best discriminated ulcer patients from controls. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2. Right Column, Lines 30-48. |
|
25. Peptic ulcers are a rare disease in childhood. |
Most children do not comprehend the gravity of life events or how the events affect them in the future. Major life events and psychological distress during childhood and adolescence might differ in some fundamental ways from adulthood. Children are comfortable in their own skin and not as effected by social expectations. Their different feelings and mindset, as compared to adults suggest they experience less stress, resulting in the rarity of peptic ulcers in children. |
Article 3, Page 35, Left Column, Lines 1-13. |
|
26. Although gastric ulcer and duodenal ulcer share something in common, they are believed to be different diseases. |
Individuals who are susceptible to gastric and duodenal ulcers belong to two genetically different populations. Table-1 fully elucidated the similarity and differences between duodenal and gastric ulcers. |
Article 2, Page 20, Left Column, Lines 6-27. |
|
27. The final stage of ulceration is a corrosive rather than an infectious process. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors, including gastric acid and pepsin, H. pylori, mechanical abrasion, and chemical erosion from medications such as NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
28. The gastric acid secretion of duodenal ulcer patients is much higher than a normal person, but only 7–8.5% of the duodenal ulcer patients are suffering from gastric ulcer simultaneously. |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid. Some individuals may have the genetic background for both gastric and duodenal ulcers and thus, they may have both types of ulcers simultaneously. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
29. Severe emotional stress may contribute to ulcer perforation and bleeding in some patients. |
The degree to which individuals suffer negative impacts from life events determined the size and depth of the nodes. A moderate stress causes small and superficial ulcers, but severe emotional stress may cause ulcer perforation and bleeding. |
Article 2, Page 18, Left Column, Lines 19-28. |
|
30. Many uncomplicated lesions heal in spite of the presence of acid gastric content, as shown by the “spontaneous” remissions of the disease and by the healed scars found at x-ray and at autopsy; however, the healing of peptic ulcer is much more rapid when the lesion is protected from the action of acid gastric juice. |
The impacts of the pathogenic nerve impulses are relieved at the ulcerated location once the distal ends of the nerves necrotize. As a result, gastric ulcers may heal up automatically via the regeneration of local tissues without treatment. Medications may attenuate the impact of local aggressive factors, such as inhibiting the hyper-secretion of gastric acid, eradicating H. pylori, increasing the resistance of the mucosa, or protecting the injured mucosa. Thus, medications may be conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 18, Left Column, Lines 30-49. |
|
31. Autopsy reports showed: 20%-29% of males and 11%-18% of females were found to have suffered from ulcers in the past or present. |
Heredity is an innate factor playing a baseline role in peptic ulcers, which predisposes a proportion of individuals in the population to an ulcer personality. Thus, not all the individuals suffer peptic ulcers. From the 1900’s to the 1950’s, men were often the direct participants of various social conflicts such as wars and financial crisis, and they were more likely to bear economical pressures than women, explains a higher percentage of males (20-29%) have suffered from ulcers in the past or at present than females (11-18%) in autopsy reports. |
Article 3, Page 37, Right Column, L12-27; Article 3, Page 37, Right Column, Lines 41-52. |
|
32. It is believed that, not only should the prognosis and assessment of ulcer have mental assessment, but the treatment without mind adjustment is also incomplete. |
A complete cure of peptic ulcers depends on the resolution of life events and/or the resolution of mental health concerns; Promoting social harmony and mind adjustment are essential etiological therapy for a complete cure of peptic ulcers without relapse. |
Article 3, Right Column, Page 38, Lines 2-7; Article 3, Page 39, Left Column, Lines 35-43. |
|
33. Peptic ulcer patients may have “ulcer personality”, such as immaturity, impulsivity, and feelings of social isolation and alienation. |
Heredity is an innate factor playing a baseline role in peptic ulcers, which predisposes a proportion of individuals in the population to an ulcer personality. |
Article 3, Page 37, Right Column, Lines 12-27. |
|
34. In a 2-year study of Pima Indians, Hesse did not find any peptic ulcer disease. |
|
|
|
35. In contrast to Pima Indians, 10% of Caucasians develop peptic ulcers. |
|
|
|
36. To date, no consistent pattern of factors, in either host or organism, has been identified that successfully predicts which infected persons will subsequently have ulcer disease. |
According to the complete picture painted in this Article 3, the occurrence of peptic ulcers is predictable if the 4 preconditions are satisfied: heredity; Hyperplasia and hypertrophy in the stomach and/or a negative life-view, psychological stress, H. pylori infection and NSAIDs usage |
Article 3, Page 37, Right Column, Line 1-Page 38, Left Column, Line 41. |
|
37. The relationship between life events stress, psychological factors and peptic ulcer diseases is not clearly established at the present time and warrants further study. |
Without the CCR, there is no benchmark to identify the cause of disease. As a result, no disease has been fully understood. Without the CCR, the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. |
Article 1, Discu, Page 9, Left Column, Lines 43-53;Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
38. Richard emphasized the different aetiology of gastric and duodenal ulcers and persons with gastric and duodenal ulcers differ epidemiologically, behaviourally, and genetically. |
Table 1 listed all the commonalties and differences between duodenal and gastric ulcers. |
Article 2, Page 20, Table 1. |
|
39. Gastric ulcer was more frequent than duodenal ulcer, 4G:1D in 1900 versus 10D:1G currently. More women than men had the disease, but now it has become reversed; from 3F:1M to 4M:1F for gastric ulcer and 10M:1F for duodenal ulcer. |
These reversions are due to the profound changes in social environments during the past century. The reversion of the sex ratio can be explained by the liberation and improved social status for women. The civilization and urbanization, etc. result in the reversion of gastric: duodenal ratio. Before 1900, the life threats or survival-related challenges and the severe shortages of supplies for the majority determined the majority of peptic ulcer cases were gastric ulcer patients. However, after 1900, especially after World War II, most of the threats to survival disappeared and the steady growth of people's living standard lead to the decreased incidence of gastric ulcers, whereas the fast rhythm of modern life, fierce social competition, and unhealthy life style, etc. primarily induce duodenal ulcers. |
Article 3, Page 31, Left Column, Line 33-Right Column, Line 11. |
|
40. Stress ulcers in the rat are primarily gastric rather than duodenal, the latter typically requiring additional artificial chemical potentiation (e.g., histamine). |
It may take ~5 years to induce the hyperplasia and hypertrophy in the human body. As a result, it is hard to duplicate this chronic pathophysiological process in the lab, thereby making it difficult to establish animal models for stress-induced duodenal ulcers. Duodenal ulcer is a chronic disease associated with the individual’s daily behaviors, and multiple psycho-neuro-endocrine organs were involved. Thus, stress-induced duodenal ulcer is hardly reproduced in animal models due to short lifespans. |
Article 1, Page 5, Left Column, Lines 14-20; Article 1, Discu, Page 9, Left Column, Lines 15-20.
|
|
The psychological stress triggering gastric ulcers is usually short-term and acute. This kind of stress can be simulated in labs and therefore, stress-induced ulcers in labs are usually gastric ulcers. |
Article 2, Page 16, Left Column, Lines 2-11. |
|
|
41. Many ulcer patients and some physicians believe that symptomatic exacerbations of peptic ulcer disease occur during or shortly after stressful events. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
42. Mental disorders (or stress) are associated with increased rates of peptic ulcer diseases. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors, which focuses more on the impact of mental health related to past life experience, made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
43. The spontaneous remissions and relapses of peptic ulcers have never been explained. |
Clinical patients suffer the relapse of peptic ulcers, because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the impact of stress caused by personality traits or negative life events has not been eliminated. Chronic stress-induced hyperplasia and hypertrophy of gastrin and parietal cells are the crux of duodenal ulcer issue, determine the spontaneous remissions and relapse of duodenal ulcer, but this psychopathological mechanism has never been elucidated in modern medicine. The etiology of peptic ulcer has never been identified, causing the problem. |
Article 1, Page 8, Right Column, Lines 7-14; Article 1, Discu, Page 9, Left Column, Lines 15-26. |
|
44. The pathophysiology of peptic ulcer has centred on an imbalance between aggressive and protective factors. |
The mechanisms of diabetes and cardiomegaly suggest that the origins of disease and the pathological changes could present in different organs. Therefore, the traditional etiological concept (The pathophysiology of peptic ulcer has centred on an imbalance between aggressive and protective factors) is not sufficient to discover the cause of disease, and peptic ulcers may not be a local disease, but a general disease due to abnormalities in other parts of the human body. |
Article 3, Page 33, Right Column, Lines 4-24. |
|
45. No single theory in history could fully explain the pathogenesis of peptic ulcers. |
Each of the single theory focused on only one area of the human body, and there is no holistic review of peptic ulcers before. Without the CCR, there is no benchmark to identify the true cause of disease. In addition, without the CCR, the methodologies for data analysis have never been established. Although each of the historical theory did make important discoveries and proved useful to understand peptic ulcers, they were overshadowed by the discovery of H. pylori. |
Article 1, Page 3, Left Column, Lines 20-29; Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
Table S6: Index of 30 elucidated H. pylori-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
46. African Enigma: The H. pylori infection rate is high (close to 100%) throughout Africa, but the prevalence of duodenal ulcer varied in different parts of the continent. |
|
|
|
47. Only the presence of duodenal ulcers, and not gastric ulcers, was associated with increasing H. pylori density. The association between gastric ulcers and H. pylori infection is less clear. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. Cases B to J explain why H. pylori density is associated with the morbidity rate of duodenal ulcers. |
Article 1, Page 7, Right Column, Lines 34-48. |
|
In gastric ulcers, it is not the total corrosive intensity of local aggressive factors, but the formation of submucous nodes that determines the occurrence of gastric ulcers. Therefore, H. pylori has a dose-effect on only duodenal ulcers, whereas gastric ulcers’ association with H. pylori is less clear. |
Article 2, Page 19, Right Column, Lines 3-12. |
|
|
48. Only 27% of symptomatic children with peptic ulcers were H. pylori positive. |
|
|
|
49. 48% of patients developed ulcers within six months of healing, but the re-infection rate after eradication was very low (<2%). |
|
|
|
50. In developing countries with uniformly high prevalence of H. pylori infection, there are marked regional differences in the prevalence of duodenal ulcers, which could not be explained by the more toxic CagA and VacA H. pylori strains. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
51. In the countries with low prevalence of H. pylori, 30%-40% or more of duodenal ulcer patients are H. pylori-negative, and the absence of H. pylori infection in early cases of duodenal ulcers was also reported. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration. Cases D, F, L, and N support the finding that in some countries, 30%-40% of duodenal ulcer 386 patients were H. pylori-negative and explain a clinical observation that up to 35% of 387 infected patients failed to respond to standard anti-H. pylori therapy. |
Article 1, Page 8, Left Column, Lines 2-16; Article 1, Page 8, Right Column, Lines 19-27. |
|
52. The role of H. pylori in peptic ulcers is controversial. |
Without the CCR, there is no benchmark to identify the cause of disease, and the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. No longer controversial after the application of the CCR. |
Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
53. ‘H. pylori is the most important aetiological factor so far described for duodenal ulcer’. |
This is a wrong statement. The hyper-secretion of gastric acid is a determinant factor in the late phase of duodenal ulceration; Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, suggesting it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duodenal ulcers. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
54. How H. pylori infection can lead to ulceration is unknown. |
This statement is based on a wrong assumption. Without the hypersecretion of gastric acid, the corrosive intensity caused by either H. pylori or NSAIDs could not reach the threshold of ulceration. H. pylori alone cannot lead to ulceration and thus, the etiology based on H. pylori infection would never be able to explain peptic ulcerations. |
Article 1, Page 7, Right Column, Lines 44-53. |
|
55. No H. pylori, No Ulcer; peptic ulcer is an infectious disease. |
These are wrong statements. Neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 38-48.
|
|
56. In spite of a high prevalence of H. pylori infection worldwide, the incidence of duodenal ulcer disease in both adults and children is low in comparison. |
Case B is applicable to most H. pylori infected individuals, but only those also impacted by the hyper-secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. |
Article 1, Page 8, Left Column, Lines 17-23. |
|
57. Kato and colleagues’ retrospective analysis found that H. pylori prevalence in gastric ulcer did not reach 50%; they concluded while H. pylori infection appears to be a risk factor in gastric ulcer, other causes are responsible for most cases. Only 56-96% of gastric ulcer patients are H. pylori-positive, so other factors must be involved. |
The formation of submucous nodes is irrelevant to H. pylori infection, but determined by only the pathogenic nerve impulses from the CNS. Without infection, gastric ulcers may occur if the individual is severely impacted by psychological stress. Therefore, more than 50% of clinical gastric ulcer patients can be H. pylori-negative. The pre-existed pathological lesions in the gastric wall due to psychological stress account for the other unidentified factors. On the other hand, because gastric ulceration is determined not by H. pylori infection, but by the formation of submucous nodes induced by psychological stress, even though the infection rate in the population is as high as 90%, only the individuals affected by psychological stress become ulcer patients, leading to the low incidence of gastric ulcers despite a high prevalence of H. pylori infection. |
Article 2, Page 19, Left Column, Lines 32-49. |
|
58. Despite the fall in prevalence of H. pylori infection, the attributable risk of H. pylori infection in peptic ulcer disease has not changed. |
Since H. pylori infection is not the cause of peptic ulcers, the attempt to explain an epidemiological observation by H. pylori infection would inevitably result in the inconsistency. |
Article 2, Page 19, Left Column, Line 49-Right Column, Line 2. |
|
59. There was a significantly higher incidence of idiopathic duodenal ulcers in the younger generation. |
The younger the individuals, the less chances they get infected with H. pylori and/or become a NSAIDs users, resulting in the significantly higher incidence of idiopathic [peptic] duodenal ulcers in the younger generation. |
Article 2, Page 19, Right Column, Line 51-Page 20, Left Column, Line 3. |
|
60. There are basically three different types of peptic ulcer: H. pylori-related peptic ulcer; NSAID-related peptic ulcer; and non-H. pylori, non-NSAID ulcer. |
This classification is because the cause of peptic ulcers has never been not identified in modern medicine. This classification overlooks the primary/decisive factor in the occurrence of duodenal ulcers, the hypersecretion of gastric acid. |
Article 1, Page 8, Right Column, Lines 14-18. |
|
61. A relatively isolated group of Australian aboriginals have virtually no H. pylori infection and hardly any peptic ulcer disease. |
|
|
|
62. Up to 20% of patients with ulcers suffer a relapse of ulcer disease despite successful eradication of their infections, suggesting that H. pylori was not the cause of their original ulcers. |
Cases D and F were caused simply by the hypersecretion of gastric acid due to psychological stress, which explain 20%-40% of patients with idiopathic ulcers (H. pylori-negative and non-NSAIDs user) and the eradication of H. pylori can not prevent the relapse of these cases. |
Article 1, Page 8, Left Column, Lines 42-46. |
|
63. Difference in virulence of H. pylori strains (cag- and cag+) has been considered as a putative explanation as to why only a minority of infected population develop peptic ulcers. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA, cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
64. H. pylori infection in rats was successful and was accompanied by a mild to moderate mucosal inflammation. After H. pylori inoculation, an ulcer was induced in the oxyntic mucosa of both infected and uninfected rats by exposing the serosal side to acetic acid. |
For those individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating that gastric acid plays a more important role than H. pylori in duodenal ulcerations. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
65. More than 95 percent of patients with duodenal ulcers and more than 80 percent of patients with gastric ulcers are infected with H. pylori. |
|
|
|
66. The corresponding ulcer areas in the H. pylori-infected rats were significantly larger in the infected than in the uninfected rats, and ulcer healing was delayed in the infected rats. Eliminating H. pylori accelerates the healing of ulcer. |
Only after the submucous nodes have come into being, could H. pylori have the chance to corrode the tissues at the site, enlarging the lesions and delaying the regeneration and rehabilitation of local tissues. Eradicating H. pylori attenuates the impact of local aggressive factors, is conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 19, Left Column, Lines 18-31; Article 2, Page 18, Left Column, Lines 42-49. |
|
67. Eradication of H. pylori in gastric ulcer patients has also been shown to be associated with a significant reduction in ulcer relapse rate, compared with those who remain infected. |
Medications, such as proton pump inhibitors for gastric acid reduction and antibiotics for H. pylori eradication, may mitigate symptoms, reduce the morbidity rate, and delay relapse to a certain degree, and many cases were diagnosed as healed, but the real cause of gastric ulcers, psychosocial stress, was not removed. As a result, relapse may occur during treatments. |
Article 2, Page 18, Right Column, Lines 3-10. |
|
68. Clinical data reported that the recurrence rate is as high as 74-80% in H. pylori positive group of duodenal ulcer patients who have healed, but the negative group is only 0-28%. The discrimination was remarkable. |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, which are representative of most clinical patients. However, the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori-negative Cases D and F, or in the H. pylori-positive Cases J and R, where the damage caused by the bacterium was not a determinant factor in ulceration. It is more common to identify cases similar to Cases G and I in clinical patients, whereas cases like Cases D, F, J and R occur less frequently, which explains the dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
69. A negative interaction between H. pylori and NSAIDs on duodenal ulcers suggests that H. pylori reduces the development of ulcers in NSAIDs users. |
H. pylori upregulates the expression of COX-2 and subsequently results in the biosynthesis of gastroprotective prostaglandin, which in turn offsets the corrosive intensity of NSAIDs and thus is conducive to the healing of NSAIDs-induced ulcers, causing ‘H. pylori reduces the development of ulcers in NSAIDs users’. |
Article 1, Page 7, Left Column, Lines 46-52. |
|
70. ~20% of peptic ulcers in the Polish population are unrelated to H. pylori and NSAIDs use (idiopathic ulcers). |
For individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
71. The prevalence of H. pylori in patients with bleeding ulcers may be 15~20% lower than in patients with non-bleeding ulcers. |
Bleeding indicates patients are more likely to be seriously impacted by psychological stress with severe hyperplasia and hypertrophy of parietal and gastrin cells as Cases F and H. pylori infection is not essential for ulceration. In contrast, non-bleeding ulcer suggests the patients are more likely to be slightly impacted by stress with mild hyperplasia and hypertrophy, and H. pylori infection is essential to increase the total corrosive intensity for the induction of ulcers as Case G. As a result, clinical bleeding ulcer patients are more likely to be Case F without H. pylori and non-bleeding patients are more likely to be Case G with H. pylori Infection. |
Article 1, Page 8, Left Column, Line 47-Right Colum, Line 7. |
|
72. The eradication of H. pylori reduces the rate of re-bleeding in patients with ulcer disease. |
The eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 41-44. |
|
73. How H. pylori infection affects gastric acid secretion is still unclear. |
The hypersecretion of gastric acid is unrelated to any of the local aggressive factors, such as H. pylori infection, NSAIDs and other medications, but potentiated by the hyperplasia and hypertrophy of one or more endocrine organs and triggered by psychological stress due to personality traits or life events. Thus, ‘H. pylori infection affects gastric acid secretion’ is a wrong assumption. |
Article 1, Page 5, Right Column, Lines 20-35. |
|
74. The incidence of peptic ulcers was higher in H. pylori-infected patients than in the H. pylori-negative group. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
75. Duodenal acid load determines whether H. pylori can cause duodenal ulcer. |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 25-35. |
|
76. The increase in H. pylori density is related to the presence of duodenal ulcer disease. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
77. H. pylori-negative duodenal ulcers were associated with a poorer prognosis mainly because of a higher rate of ulcer and symptom relapse. |
To reach the ulceration threshold without the corrosive intensity from H. pylori, the hypersecretion of gastric acid needs to be higher in H. pylori-negative patients. The higher hypersecretion in Cases D and F indicates more severe negative impacts from psychosocial stress than in Cases G and I. Additionally, the damage from H. pylori can be relieved by antibiotics, as in Cases G and I, decreasing the corrosive intensity in these patients, whereas Cases D and F cannot achieve the same therapeutic effect. Therefore, there is a poorer prognosis and a higher relapse rate in H. pylori-negative patients. |
Article 1, Page 8, Left Column, Lines 31-41. |
|
78. When H. pylori persisted, 61% of duodenal ulcers healed and 84% relapsed. When H. pylori was cleared 92% of ulcers healed and only 21% relapsed during the 12 months follow-up period. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity and duodenal ulceration is caused by the total corrosive intensity, the higher density of H. pylori, the higher total corrosive intensity. As a result, H. pylori infection exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. In contrast, the eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 34-44. |
|
79. Jyotheeswaran and colleagues from greater Rochester, New York, reported a 48% prevalence of H. pylori-negative duodenal ulcers in white patients and 15% in non-white patients, with an overall negative prevalence of 39%. Parsonnet’s meta-analysis indicates the overall prevalence of H. pylori-negative duodenal ulcers is 40%. |
For those individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients.
|
Article 1, Page 5, Right Column, Lines 36-52. |
|
80. A review by van der Voort and colleagues suggests that existing data are consistent with a causal role for H. pylori in stress ulcer formation. |
A statement originated from wrong etiology. ‘A causal role for H. pylori in stress ulcer’ indicates that without stress, H. pylori alone can not induce ulcer. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duodenal ulcer. Case B in Figure 2 is applicable to most H. pylori infected individuals, but only those also impacted by the hyper-secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. That explained the wrong statement “a causal role for H. pylori in stress ulcer formation”. |
Article 1, Page 5, Right Column, Lines 43-52. Article 1, Page 8, Left Column, Lines 17-25. |
|
81. Barry Marshall drank a concoction made from cultured H. pylori and came down with gastritis that could be cured with antibiotics. |
|
|