
Effects of Interpersonal Psychotherapy on Postpartum Depression among Females at Tertiary Care Hospital Lahore
Sehrish Arshad1*, Muhammad Afzal2, Hajra Sarwar3
1Doctors Hospital College of Nursing and Allied Health Sciences, Lahore, Pakistan
2Director Academics Faculty of Allied Health Sciences, University of Lahore, Pakistan
3University of Lahore, Pakistan
Abstract
Introduction: Postpartum depression (PPD) is a major public health issue among females after giving birth to the baby, characterized by low mood, feeling of guilt and suicide. When left untreated, it has the potential for a profound negative impact on mothers, children and families. The efficacy of interpersonal psychotherapy (IPT) in addressing depression has been well-documented. However, the impact of IPT on PPD remains inadequately substantiated, particularly within the context of Pakistan, where data pertaining to its effectiveness remains limited.
Objective: The aim of study was to assess the level of depression in postpartum females and evaluate the effects of IPT on PPD among females at tertiary care hospital Lahore.
Methods: A Randomized controlled trial (RCT) was conducted at the Services Hospital Lahore from September 2021 to the same month in 2023. Subjects (n=110) were screened using the hamilton depression rating scale (HDRS) and divided equally in intervention group and control group to get eight sessions of individual based IPT versus routine care. Data was analyzed using SPSS version 21, intergroup comparison was done by Mann Whitney U test for intra group comparison Wilcoxon Signed Rank test was used, with 95% Confidence Interval (CI) and 5% level of significance. Significance of result showed with p value <0.05.
Results: Prevalence of PPD among female was observed 82%. Upon receiving IPT, females exhibited a statistically significant reduction (p<0.001) in scores indicative of mild depression, from 48 (87.3%) to 5(9.1%), as well as for moderate depression, from 7(12.7%) to 1(1.8%). Furthermore, following the IPT sessions, marked improvements were noted within the intervention group across various domains including depressed mood p<0.001, CI (0.000, 0.027), feelings of guilt p<0.001, CI (0.000, 0.027), early night insomnia p<0.008, CI (0.000, 0.043), impaired work and activities p<0.05, CI (0.072, 0.200), and insight p<0.001, CI (0.000, 0.027). Conversely, the control group did not exhibit any significant alterations in these parameters.
Conclusion: The results indicate a concerning prevalence rate of PPD among the study sample with many cases remaining undiagnosed and untreated. More positively, the study demonstrates the potential of IPT as an effective method to mitigate mild to moderate PPD. This research suggests the incorporation of IPT into therapeutic models could result in timely, potentially preventive interventions and lessen the occurrence of severe complications.
Introduction
Background
Postpartum depression (PPD) is a significant challenge for maternal morbidity, if it remains untreated, PPD may increase the risk of psychosis, suicide and in rare cases infanticide. PPD has negative consequences for the social relationship of females and for the development of their infant. It starts at any time with in the first year of delivery and is common between 4-6 weeks after giving birth and can last for several years.1 Symptoms vary from low mood, loss of interest in activities, guilt, insomnia, hopelessness, anger, low self-esteem and suicidal ideation.2 However, many factors lead to PPD such as physiological, psychological, social and cultural but the most common factor affecting primigravida females is “Role transition” where after becoming a mother, women face challenges like care of newborn, redefine relationship with spouse and family members and at work place that can lead to depression among them.3 Additionally, mother infant bonding may be reduced due to maternal depression, which affects the behavior of mother, and can damage the mental, as well as behavioral and emotional progress of children.4
According to a systematic review and meta-analysis, including a total of 565 studies from eighty different countries, the prevalence of PPD is estimated at 17.22% (95% CI 16.00, 18.51) of the world’s population. Additionally, rates were higher in geographical region of Asia (3.5% to 63.3%), and at local level highest prevalent countries among Asia are Afghanistan (90 to 93%) and Pakistan (28 to 63%).4 A cross-sectional study conducted at three major tertiary care setups of Sindh in Pakistan, sample size was 357 and prevalence of PPD reported as 28 to 63%.5 Moreover, an observational cross-sectional survey targeting a sample of 444 in Jazan was conducted to see prevalence of PPD that was found 75.7%.6 According to another study conducted on 109 postpartum females diagnosed with PPD, it was estimated that 15-85% women experience PPD within 10 days of giving birth.7
There are many contributing factors for PPD including biological factors (Obesity, medical disorders, family history of PPD, hormonal changes) psychological factors (past psychiatric history, low self-esteem, dependency level, coping mechanism), social factors (marital conflicts, lower social class, poor support of parents, smoking and employment status), obstetric factors (multiple births, complication during pregnancy, abortion, medical disorder of baby, premature baby and unplanned pregnancy), cultural factors (female baby gender, different tradition of care of baby, believes and food). All above mentioned factors have major role in developing the PPD among females.8
First line treatment for PPD is pharmacological treatment but women refuse to take medicine due to lactation exposure to the babies and prefer the non-pharmacological measures.9 IPT is a limited and focused procedure to treat the depressive disorders. IPT targets the problem in four key areas interpersonal conflict, transition in role, grief and deficit in relationship, and addresses them by using different techniques like clarification, communication, supportive listening, role play and encouragement.10 There are three phases of IPT, initial, intermediate and final phase. In initial phase therapist builds a relationship with the client and identifies the issue, in the intermediate phase, the therapist applies different techniques to resolve the issue, and in the final phase, the therapist plans for termination of therapy and relapse prevention.11 There is evidence to support the use of psychosocial strategies such as peer support and nondirective counseling in PPD. Nondirective counseling by professionals or paraprofessionals may reduce symptoms of PPD in females.12
Role transition in primigravida females being a new parent is discussed in this study. It involved adopting a new role, learning new skills, increase responsibility, more stress and less sleep, while maintaining the existing responsibilities and relationships. Patient may feel that they are being pulled in many directions that may increase demand which can result in low self-esteem and confusion in role. Thus, the aim of IPT is to allow the patient to express her positive and negative feelings about the new role, explores the benefits and makes strategies to adopt the new role and reduce the level of depression.13 PPD occurs due to major life changes (giving birth to a baby), hormonal imbalance, birth trauma, withdrawal from job and crises in life (divorce, death of loved ones). One of the most effective method to deal with PPD related to role transition is to help the females to accept and adopt the changing roles (e.g. being mother) to overcome their mental disorders.14
Thus, the objective of study was to assess the level of depression in postpartum females and evaluate the effects of IPT on PPD among females at tertiary care hospital Lahore.
Hypothesis
H0: There is no effect of IPT on PPD among females who receive IPT as compared to control group at tertiary care hospital Lahore.
H1: There is an effect of IPT on PPD among females who receive IPT as compared to control group at tertiary care hospital Lahore.
Materials and Methods
Study Population
Screening was done in post-obstetric departments of services hospital Lahore Pakistan. First of all eligibility criteria was applied, participants included in the study were only primigravida females, undergoing postpartum period (within six weeks of spontaneous vaginal delivery or cesarean section), age range between 18-35 years. Moreover, screening done by Hamilton Depression Rating Scale (HDRS) to select participants with mild to moderate depression 8-23 (15.09% to 43.39%). Hence HDRS has total of 53 scores, mild depression is characterized by score falling within the range of 8-16 (15.09% to 30.18%) and for moderate depression 17-23(32.08% to 43.39%). In alignment with the research eligibility targeting participants exhibiting mild to moderate depression, we enrolled subjects with level of depression 8-23(15.09% to 43.39%) representing mild to moderate depression. Patients excluded from study were multigravida females, have some medical issues (diabetes mellitus, hypertension), mental disorders (severe depression, psychosis, mania & bipolar disorder), substance abuse, fetal issues (preterm <37 weeks, still birth & severe medical illness) and female has death of family member with in last six months.
Sample Size
Sample size calculated with 95% confidence interval and 80% power of test. Expected mean depression score in group A (Intervention group) as 12.6 ± 7.0 and in group B (Control group) as 16.4 ± 6.5.15 Total sample size was 100, after adding 10% drop out rate sample size was 110, equally divided in control group (55) and in intervention group (55).
Attrition Rate
We planned to enroll more subjects to compensate the attrition rate. There was a dropout rate in our study. Total ten subjects dropped out in both groups at different time intervals. At the end of intervention sample size remained same in intervention group as well as in control group.
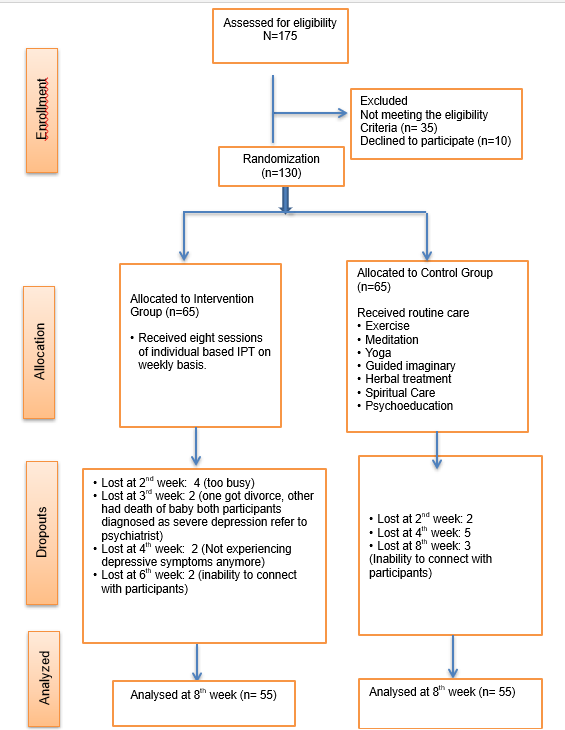
Figure 1: Flow Diagram of Participants
Data Collection Procedure
After getting permission from ethical committees of respective organization data collection was started from 4thApril, 2023. Those willing to participate in the study were asked to fill and sign the consent form. Simple random sampling technique used to select participants according to eligibility criteria. Afterwards, HDRS consist of 17 items used to assess the severity of symptoms of depression. Structured questions were asked by face to face interview to obtain information regarding socio demographic characteristics (age, education, profession, mode of delivery) others questions were categories of HDRS (depressed mood, feeling of guilt, suicide etc.) to assess the severity of symptoms and level of depression of study participants. Eight sessions of individual based IPT given to intervention group whereas control group received only routine care. Post data collected from 6th October 2023 from both groups’ control group as well as intervention group.
Study Design, Randomization and Masking
Randomized controlled trial (RCT) used as study design. Researcher controlled the context by controlling the confounding factors that may effect on study variables by setting the eligibility criteria like age of participants, medical disorders (diabetes, hypertension), death of family members within last six months. Block Randomization is used to ensure the equal sample size of both groups over time and control the selection bias. Excel sheets are used to generate the blocks of equal size of study participants. There were 130 participants, number of interventions were 2 so made blocks (2, 4, 6, 8, 10) and put equal number of participants over there. In this study 10 blocks were formulated and 13 subjects (130/10) randomly put in each group by pressing the rand= () on the excel sheet, then by using the simple random sampling technique 5 blocks has been chosen for intervention group and 5 blocks for control group. Moreover, single blinding applied to control the selection bias. In this study only “Participants” were masked, they were unaware in which group they were selected intervention group or control group. Selection was done by closed envelope method. Manipulation was done by giving IPT to the intervention group and withholds it to the control group.
Ethical Consideration
The Research Ethics Committee (REC) of university of Lahore and Institutional Review Board (IRB) of services hospital Lahore under the registration number REC-UOL-353-04-2023 and IRB/2023/1066/SIMS have approved this study prospectively. Consent form in Urdu version signed by each participant prior to conduct the study. Risk and benefit of study discussed with participants. Confidentiality maintained by not showing the names of participants but they were given codes like pre int (pre intervention), Post int (Post Intervention), Pre cont (Pre Control) & Post Cont (Post Control).
Control Group
Control group received only routine care provided by the health care providers in their respective department or by their selves, most commonly used methods were yoga, exercise, meditation, guided imaginary, herbal medicines, spiritual treatment, prayers and psychoeducation. They were not given IPT to get fair comparison between control group and intervention group.
Intervention Group
Intervention group used routine care in addition they were given eight sessions of individual based IPT on weekly basis. Customized plan made according to need of the patient, intervention module consisted of booklet and videos. Each session took almost 30 min to 45 min. IPT was given into three phases, initial phase, middle phase and termination phase. In initial phase (1st week), therapeutic alliance built with client, introduction of IPT and benefits discussed and issue related to role transition were identified. In middle phase (2-6 weeks) different techniques used to resolve the issue like psychoeducation, role play and communication. Most common issues identified in primigravida females regarding role transition were sleep deprivation, feeding difficulties, care of baby, anger and lack of interpersonal skills. In termination phase (7-8 weeks) patients were assured about termination of therapy and guided about the ways for relapse prevention.
Training of Researcher
The researcher who was a nurse had clinical expertise more than twelve years in different specialized fields (Pediatric, NICU, medical ICU, gynecology, obstetric & clinical psychology) of tertiary care hospital Lahore. To enhance the further skills, she had completed diploma in advance psychology and attended different workshops on IPT. Additionally, for the excellence of performance intervention given under supervision of expert clinical psychologist.
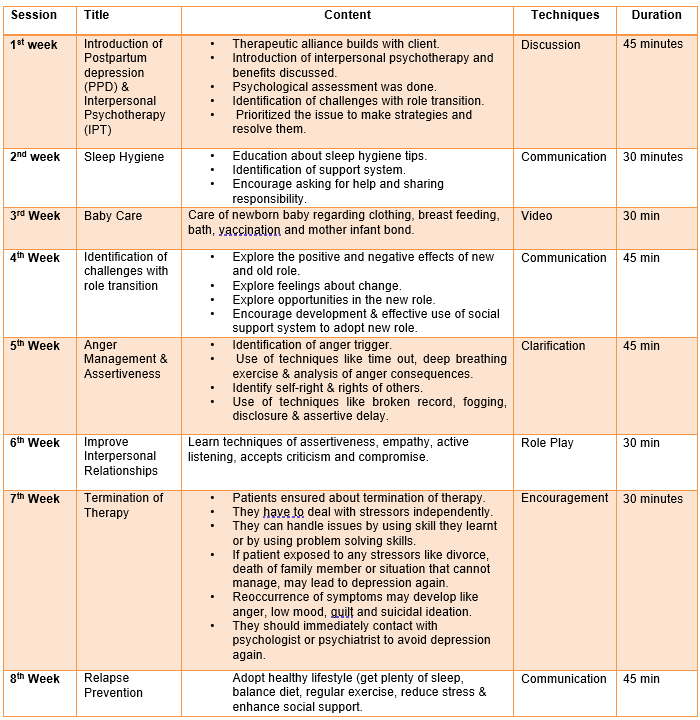
Figure 2: Intervention Plan
Research Tool
HDRS used as research tool. Original version has a total of 17 items with minimum 0 to maximum 53 scores. Postpartum depression measured by following criteria, no depression <8 (<15.09%), mild depressions 8-16 (15.09%-30.18%), moderate depression 17-23 (32.08% - 43.39%) and severe depression > 24 (>45.28 %). Hamilton rating scale for depression is the valid and reliable instrument for the assessment of severity of depression. It showed good internal consistency (Cronbach alpha 0.71), good test-retest reliability and good inter-rater reliability. It was regarded as useful tool in clinical practice and research.16
Statistical Analysis
Quantitative variables such as HDRS categories expressed as mean ± SD, while categorical variables such as demographic characteristics presented as frequency and percentage. The association between categorical variables assessed using the chi-square test. Normality of data distribution evaluated through Shapiro-Wilk and Kolmogorov-Smirnov tests with significance determined at (p > 0.05) indicative of a normal distribution. Mean differences between groups analyzed using the Mann-Whitney U test, while within-group comparisons conducted using the Wilcoxon Signed Rank test. Data analysis performed using SPSS version 21 with 95% of CI and 5% margin of error. The statistical significance level accepted as (p<0.05).
Results
Prevalence of Postpartum Depression
Prevalence of PPD calculated as the number of postpartum females diagnosed with PPD using the HDRS out of all females enrolled into study and expressed as a percentage 145/175=82%.
Sociodemographic Variables
According to socio demographic characteristics maximum number of females fall under age of 19-26, 39(70.9%) in intervention group and 37(67.3%) in control group, most of them were matric by their qualification in intervention group 19(34.5%) and control group 17(30.9%) respectively. There were 54(98.2%) subject housewives and only 1(1.8%) female reported as working woman in both groups. Only 2(3.6%) females reported as SVD in both groups because primigravida females most probably have to undergone C-sections. Socio demographic data has shown no significant difference in comparison to control group as well as intervention group. (Table 1)
Table 1: Comparison of Sociodemographic characteristics of control group (n=55) and Intervention group (n=55)
|
S/N |
Characteristics |
Control group n (%) |
Intervention group n (%) |
Test value |
p value |
|
|
1 |
Age:
|
<18 |
2(3.6%) |
4(7.3%) |
0.719 |
0.869 |
|
19-26 |
39(70.9%) |
37(67.3%) |
||||
|
27-34 |
12(21.8%) |
12(21.8%) |
||||
|
>35 |
2(3.6%) |
2(3.6%) |
||||
|
2 |
Education:
|
Middle or lower |
15(27.3%) |
16(29.1%) |
0.372 |
0.946 |
|
Matric |
19(34.5%) |
17(30.9%) |
||||
|
Intermediate |
9(16.4%) |
10(18.2%) |
||||
|
Graduate or above |
12(21.8%) |
12(21.8%) |
||||
|
3 |
Profession:
|
Housewife |
54 (98.2%) |
54 (98.2%) |
0.000 |
1.000 |
|
Working women |
1(1.8%) |
1(1.8%) |
||||
|
4 |
Mode of Delivery: |
SVD |
2(3.6%) |
2(3.6%) |
0.000 |
1.000 |
|
C-sections |
53(96.4%) |
53(96.4%) |
||||
n (number), % (percentage), test value (chi square value), p value<0.05(significant)
Level of Depression in Control group and Intervention group
In intervention group there were 48 (87.3%) females with mild depression after getting eight sessions of IPT remained 5(9.1%) and females with moderate depression were 7 (12.7%) remained 1(1.8%). Whereas, in control group there were 51(92.7%) females with mild depression after using routine care remained 20(36.4%) but with moderate depression there were only 4 (7.3%) females raised their level from mild to moderate depression 14(25.5%). However, only 1 (1.8%) patient reported severe depression in both groups intervention as well as control group. Significant difference has seen in intervention group before and after IPT p<0.001 but no significant difference has seen in control group p=0.428. (Table 2)
Table 2: Level of postpartum depression (PPD) in Control group and Intervention group before and after intervention
|
Depression Level |
Control Group (n=55) |
Intervention Group (n=55) |
||||||
|
Pre-N (%age) |
Post N (%age) |
T Value |
p Value |
Pre-N (%age) |
Post N (%age) |
T Value |
p Value |
|
|
No Depression |
0 (0%) |
20(36.4%) |
0.799 |
0.428 |
0 (0%) |
48(87.3%) |
18.517 |
0.000 |
|
Mild Depression |
51(92.7%) |
20(36.4%) |
48 (87.3%) |
5(9.1%) |
||||
|
Moderate Depression |
4 (7.3%) |
14(25.5%) |
7 (12.7%) |
1(1.8%) |
||||
|
Severe Depression |
0 (0%) |
1(1.8%) |
0 (0%) |
1(1.8%) |
||||
T Value: Paired T Test value, p value <0.05 Significant
Effects of Interpersonal Psychotherapy (IPT)
According to data, pre-intervention difference between control group and intervention group in terms of decrease level of depression determined non-significant. Only four variables showed statistically significant difference between intervention group and control group, feeling of guilt p<0.003, CI (0.000,0.027), insomnia at midnight p<0.008, CI (0.000,0.027), retardation p<0.015 CI (0.000,0.027) and general somatic symptoms p<0.016, CI (0.007,0.084) Table 3 (Part A). Whereas, the post intervention difference between control group and intervention group in terms of decrease level of depression determined statistically significant Table 3 (Part B). Moreover, in comparison of pre and post score within the control group, data showed no statistically significant difference Table 4 (Part A). While, in comparison of pre and post therapy scores in intervention group the difference was statistically significant Table 4 (Part B).
In accordance with the post intervention of IPT, while the fourteen out of seventeen variables found statistically significant, depressed mood p<0.001, CI (0.000,0.027), feeling of guilt p<0.001, CI (0.000, 0.027), insomnia early night p<0.008 ,CI (0.000,0.043) and midnight p<0.001, CI (0.000, 0.027) and early morning p<0.001,CI (0.000, 0.027), retardation p<0.000, CI (0.000, 0.027), work and activities p<0.052, CI (0.072, 0.200), agitation p<0.001, CI (0.000, 0.027) anxiety psychic p<0.049 CI, (0.024, 0.121), somatic p<0.001, CI (0.000,0.027) and somatic symptoms p<0.001, CI (0.000, 0.027), genital symptoms P<0.005, CI (0.000, 0.027), loss of weight p<0.028,CI (0.000, 0.043) and insight p<0.001, CI (0.000, 0.027) Table 3 (Part B).
In the comparison to the control group before and after routine care only four variables showed the statistical significant difference insomnia early night p<0.015, CI (0.001, 0.071), insomnia early morning p<0.014, CI (0.000, 0.043), work and activities p<0.026, CI (0.031, 0.133) anxiety psychic p<0.0056, CI (0.000, 0.027), general somatic symptoms p<0.017,CI (0.000, 0.058) and loss of weight p<0.028, CI (0.012, 0.097) Table 4 (Part A). Furthermore, in comparison of intervention group before and after intervention statistically significant difference was seen in term of reduction in depressive symptoms; depressed mood, suicide, insomnia early morning, retardation, agitation, anxiety psychic, somatic general somatic disorders and insight p<0.001, CI (0.000, 0.020), loss of weight p<0.03, CI (0.080, 0.020) showed significant of results. Whereas, suicide, work and activities and hypochondriasis not showed statistically significant difference Table 4 (Part B).
Table 3: Intergroup comparison of postpartum depression (PPD) scores among females in control group and Intervention group by using Mann Whitney U test
Pre-intervention (Part A):
|
S/N |
Questions: |
Groups |
Mean±SD |
Mean Rank |
Mann Whitney U Test |
Confidence Interval 95% Lowe-Upper |
p value |
|
1 |
Depressed Mood |
Control Intervention |
0.80 ±0.48 0. 91±0.59 |
53.64 57.36 |
1410.000 |
0.361-0.548 |
0.420 |
|
2 |
Feelings of Guilt |
Control Intervention |
0.67 ±0.51 0.95±0.36 |
48.30 62.70 |
1116.500 |
0.000-0.027 |
0.002 |
|
3 |
Suicide |
Control Intervention |
0.09 ±0.29 0.13±0.47 |
55.45 55.55 |
1510.000 |
0.973-1.000 |
0.976 |
|
4 |
Insomnia early night |
Control Intervention |
1.25 ± 0.58 1.42 ±0.53 |
51.71 59.29 |
1304.000 |
0.095- 0.233 |
0.152 |
|
5 |
Insomnia mid night |
Control Intervention |
0.93± 0.42 1.18 ± 0.55 |
49.28 61.72 |
1170.500 |
0.000- 0.027 |
0.007 |
|
6 |
Insomnia early morning |
Control Intervention |
1.56 ±0.60 1.45± 0.63 |
58.05 52.95 |
1372.000 |
0.317-0.501 |
0.337 |
|
7 |
Work and activities |
Control Intervention |
0.75 ±0.48 0.71±0.46 |
56.35 54.65 |
1465.500 |
0.800-0.928 |
0.721 |
|
8 |
Retardation |
Control Intervention |
0.75 ± 0.48 0.9±0.36 |
50.23 60.77 |
1222.500 |
0.000- 0.027 |
0.014 |
|
9 |
Agitation |
Control Intervention |
0.82 ± 0.47 0.95± 0.30 |
52.04 58.96 |
1322.000 |
0.037- 0.145 |
0.083 |
|
10 |
Anxiety Psychic |
Control Intervention |
1.04 ±0.63 1.20 ±0.52 |
51.82 59.18 |
1310.000 |
0.087- 0.222 |
0.133 |
|
11 |
Anxiety Somatic |
Control Intervention |
0.98 ± 0.45 0.96±0.33 |
55.93 55.07 |
1489.000 |
0.973-1.000 |
0.823 |
|
12 |
Somatic symptoms |
Control Intervention |
0.49 ±0.57 0.65±0.64 |
51.93 59.07 |
1316.000 |
0.181-0.346 |
0.187 |
|
13 |
General Somatic symptoms |
Control Intervention |
0.800 ± 0.40 0.96±0.27 |
51.10 59.90 |
1270.500 |
0.007-0.084 |
0.015 |
|
14 |
Genital Symptoms |
Control Intervention |
0.11± 0.31 0.13± 0.34 |
55.00 56.00 |
1485.000 |
0.973-1.000 |
0.769 |
|
15 |
Hypochondriasis |
Control Intervention |
0.13± 0.43 0.15±0.49 |
55.05 55.95 |
1487.500 |
0.810-0.935 |
0.774 |
|
16 |
Loss of weight |
Control Intervention |
0.51 ±0.99 0.25±0.058 |
57.58 53.42 |
1398.000 |
0.317- 0.501 |
0.350 |
|
17 |
Insight |
Control Intervention |
0.96 ±0.51 0.98±0.13 |
54.95 56.05 |
1482.000 |
0.508-0.692 |
0.760 |
Questions: HDRS categories, ± mean, Standard Deviation, p<0.05 significant
Post intervention (Part B):
|
S/N |
Questions: |
Groups |
Mean±SD |
Mean Rank |
Mann Whitney U Value |
Confidence Interval 95% Lowe-Upper |
p value |
|
1 |
Depressed Mood |
Control Intervention |
0.69 ± 0.61 0.18 ± 0.55 |
68.60 42.40 |
792.000 |
0.000-0.027 |
0.000 |
|
2 |
Feelings of Guilt |
Control Intervention |
0.76 ±0.63 0.27±0.45 |
66.82 44.18 |
890.000 |
0.000-0.027 |
0.000 |
|
3 |
Suicide |
Control Intervention |
0.13 ±0.336 0.13±0.51 |
56.87 54.13 |
1437.000 |
0.434-0.621 |
0.385 |
|
4 |
Insomnia early night |
Control Intervention |
1.15 ±0 .59 0.87±0.43 |
61.96 49.04 |
1157.000 |
0.000-0.043 |
0.007 |
|
5 |
Insomnia mid night |
Control Intervention |
0.96 ±0.57 0.31±0.47 |
70.74 40.26 |
674.500 |
0.000-0.027 |
0.000 |
|
6 |
Insomnia early morning |
Control Intervention |
1.40 ±0.59 0.75±0.55 |
69.72 41.28 |
730.500 |
0.000-0.027 |
0.000 |
|
7 |
Work and activities |
Control Intervention |
0.65 ± 0.48 0.82±0.39 |
51.00 60.00 |
1265.000 |
0.072-0.200 |
0.053 |
|
8 |
Retardation |
Control Intervention |
0.80 ±0 .59 0.11±0.42 |
72.47 38.53 |
579.000 |
0.000-0.027 |
0.000 |
|
9 |
Agitation |
Control Intervention |
0.93 ±0 .66 0.38±0.59 |
67.41 43.59 |
857.500 |
0.000-0.027 |
0.000 |
|
10 |
Anxiety Psychic |
Control Intervention |
0.89 ±0 .65 0.65±0.78 |
61.02 49.98 |
1209.000 |
0.024-0.121 |
0.048 |
|
11 |
Anxiety Somatic
|
Control Intervention |
0.85 ±0.59 0.33±0.55 |
68.13 42.87 |
818.000 |
0.000-0.027 |
0.000 |
|
12 |
Somatic symptoms |
Control Intervention |
0.58 ± 0.65 0.09±0.29 |
66.73 44.27 |
895.00 |
0.000-0.027 |
0.000 |
|
13 |
General Somatic symptoms |
Control Intervention |
0.600 ±0.56 0.42±0.50 |
59.92 51.08 |
1269.500 |
0.080-0.211 |
0.096 |
|
14 |
Genital Symptoms |
Control Intervention |
0.18 ±0.39 0.02±0.13 |
60.00 51.00 |
1265.000 |
0.000-0.027 |
0.004 |
|
15 |
Hypochondriasis |
Control Intervention |
0.07 ±0.26 0.04±0.19 |
56.50 54.50 |
1457.500 |
0.556-0.735 |
0.403 |
|
16 |
Loss of weight |
Control Intervention |
0.31±0 .69 0.07±0.26 |
59.61 51.39 |
1286.500 |
0.000-0.043 |
0.027 |
|
17 |
Insight |
Control Intervention |
0.94 ±0.48 0.07±0.33 |
77.21 33.79 |
318.500 |
0.000-0.027 |
0.000 |
Questions: HDRS categories, ± mean, Standard Deviation, p<0.05 significant
Table 4: Intragroup comparison of postpartum depression (PPD) scores among females before and after intervention in control group and intervention group by using Wilcoxon Signed Rank Test
Control Group (Part A):
|
S/N |
Questions: |
Groups |
Mean±SD |
Mean Rank |
Confidence Interval 95% Lowe-Upper |
p value |
|
1 |
Depressed Mood |
Before After |
0.80 ±0.48 0 .69 ± 0.61 |
5.50 5.50 |
0.065-0.190 |
0.058 |
|
2 |
Feelings of Guilt |
Before After |
0.67 ±0.51 0.76 ±0.63 |
5.00 5.00 |
0.110-0.254 |
0.096 |
|
3 |
Suicide |
Before After |
0.09 ±0.29 0.13 ± 0.336 |
1.50 0.00 |
0.508-0.692 |
0.157 |
|
4 |
Insomnia early night |
Before After |
1.25 ±0 .58 1.15 ± 0.59 |
0.00 3.50 |
0.001-0.071 |
0.014 |
|
5 |
Insomnia mid night |
Before After |
0.93± 0.42 0.96 ±0.57 |
4.50 4.50 |
0.634-0.802 |
0.480 |
|
6 |
Insomnia early morning |
Before After |
1.56 ±.60 1.40 ±.59 |
7.00 7.00 |
0.000-0.043 |
0.013 |
|
7 |
Work and activities |
Before After |
0.75 ±0.48 0.65 ± 0.48 |
0.00 3.00 |
0.031-0.133 |
0.025 |
|
8 |
Retardation |
Before After |
0.75 ±.048 0.80 ± 0.59 |
8.89 8.00 |
0.462-0.647 |
0.491 |
|
9 |
Agitation |
Before After |
0.82 ±0.47 0.93 ± 0.66 |
9.50 9.50 |
0.240-0.415 |
0.157 |
|
10 |
Anxiety Psychic |
Before After |
1.04 ±0.63 0.89 ± 0.65 |
0.00 4.50 |
0.000-0.027 |
0.005 |
|
11 |
Anxiety Somatic |
Before After |
0.98 ±0 .45 0.85 ±0.59 |
7.00 7.70 |
0.117-0.264 |
0.090 |
|
12 |
Somatic symptoms |
Before After |
0.49 ±0.57 0.58 ± 0.65 |
6.00 6.00 |
0.206-0.376 |
0.132 |
|
13 |
General Somatic symptoms |
Before After |
0.800 ± 0.40 0.600 ±0.56 |
11.00 11.00 |
0.000-0.058 |
0.016 |
|
14 |
Genital Symptoms |
Before After |
0.11±0 .31 0.18 ±0.39 |
3.50 3.50 |
0.214-0.386 |
0.102 |
|
15 |
Hypochondriasis |
Before After |
0.13±0.43 0.07 ±0.26 |
2.00 2.67 |
0.361-0.548 |
0.257 |
|
16 |
Loss of weight |
Before After |
0.51 ±0.99 0.31± 0.69 |
2.50 4.79 |
0.012-0.097 |
0.027 |
|
17 |
Insight |
Before After |
0.96 ±0.51 0.94 ±0.48 |
2.00 2.00
|
0.973-1.000 |
0.564 |
Questions: HDRS categories, ± mean, Standard Deviation, p<0.05 significant
Intervention Group (Part B):
|
S/N |
Questions: |
Groups |
Mean±SD |
Mean Rank |
Confidence Interval 95% Lowe-Upper |
p value |
|
1 |
Depressed Mood |
Before After |
0.91±0.59 0.18 ±0 .55 |
40.00 20.53 |
0.000-0.020 |
0.000 |
|
2 |
Feelings of Guilt |
Before After |
0.95±0.36 0.27±0.45 |
21.00 21.00 |
0.000-0.020 |
0.000 |
|
3 |
Suicide |
Before After |
0.13±0.47 0.13±0.51 |
4.83 3.38 |
0.98-1.00 |
0.931 |
|
4 |
Insomnia early night |
Before After |
1.42 ±0.53 0.87±0.43 |
14.10 11.50 |
0.000-0.020 |
0.000 |
|
5 |
Insomnia mid night |
Before After |
1.18 ± 0.55 0.31±0.47 |
23.16 19.50 |
0.000-0.020 |
0.000 |
|
6 |
Insomnia early morning |
Before After |
1.45±0 .63 0.75±0.55 |
19.64 17.0 |
0.000-0.020
|
0.000 |
|
7 |
Work and activities |
Before After |
0.71±0.46 0.82±0.39 |
11.50 11.50 |
0.227-0.373 |
0.201 |
|
8 |
Retardation |
Before After |
0.9±0.36 0.11±0.42 |
47.50 24.01 |
0.000-0.020
|
0.000 |
|
9 |
Agitation |
Before After |
0.95±0.30 0.38±0.59 |
17.00 17.00 |
0.000-0.020 |
0.000 |
|
10 |
Anxiety Psychic |
Before After |
1.20 ±0.52 0.65±0.78 |
21.31 19.50 |
0.000-0.020 |
0.000 |
|
11 |
Anxiety Somatic
|
Before After |
0.96±0.33 0.33±0.55 |
21.55 21.00 |
0.000-0.020 |
0.000 |
|
12 |
Somatic symptoms |
Before After |
0.65±0.64 0.09±0.29 |
14.50 0.00 |
0.000-0.020 |
0.000 |
|
13 |
General Somatic symptoms |
Before After |
0.96±0.27 0.42±0.50 |
17.50 17.50 |
0.000-0.020 |
0.000 |
|
14 |
Genital Symptoms |
Before After |
0.13±0.34 0.02±0.13 |
4.50 4.50 |
0.62-0.007 |
0.034 |
|
15 |
Hypochondriasis |
Before After |
0.15±0.49 0.04±0.19 |
3.60 3.00 |
0.316-0.127 |
0.096 |
|
16 |
Loss of weight |
Before After |
0.25±0.58 0.07±0.26 |
5.00 6.22 |
0.080-0.020 |
0.029 |
|
17 |
Insight |
Before After |
0.98±0.13 0.07±0.33 |
26.50 26.50 |
0.000-0.020 |
0.000 |
Questions: HDRS categories, ± mean, Standard Deviation, p<0.05 significant
Discussion
Our study suggests the primary findings of high prevalence (82%) of PPD among primigravida females. Moreover, IPT found very effective to reduce the level of mild to moderate depression among postpartum females. Females received IPT decreased their level for mild depression from 48 (87.3%) to 5(9.1%) and for moderate depression 7 (12.7%) to 1(1.8%) and showed highly significance of result p<0.001. Favorable result of IPT supports its use for the intervention of PPD and prevent from further complications.
The prevalence of PPD among females in this study was observed to be 82%, a rate potentially influenced by several contributing factors. Notably, the exclusive inclusion of primigravida females as study subjects, known to exhibit heightened susceptibility to PPD, may have contributed to this elevated prevalence. Furthermore, the timing of data collection, primarily conducted within the initial day following childbirth, may have accentuated the prevalence of certain postpartum challenges such as pain, sleep deprivation, and difficulties in infant care. Moreover, within the context of Pakistan's status as a developing nation characterized by lower socioeconomic conditions, females may experience a heightened vulnerability to PPD compared to their counterparts in more developed regions. A study showed the same result that PPD was more common among developing countries as compared to develop ones, range from 1.9% to 82.1%.28 Yet another study showed that 15-85% women out of 109 study participants experienced PPD within ten days of giving birth.7 A study conducted in Semey Kazakhstan showed that global prevalence of PPD was 0.5 to 63.3%.17 According to a systematic review and meta-analysis of eighty different countries prevalence of PPD varied in Asian countries ranged from 9-60%.18 Moreover, according to different studies prevalence of PPD has seen more common among primigravida as compared to the multigravida females.19,20,21
However, depression level in postpartum females after getting eight sessions of IPT decreased significantly as compared to control group. There were 48 (87.3%) females reported as mild depression in intervention group decreased their level of depression 5(9.1%) and 7 (12.7%) females with moderate depression decreased their level of depression 1(1.8%) and showed highly significance of result p<0.001. Similar result has seen in research conducted in 36 Canadian public health regions rural and urban settings to examine the effectiveness of nurse-delivered telephone based IPT for postpartum depression. Women experiencing postpartum depressive symptoms (EPDS score >12) were study subjects (n=241). At twelve weeks of IPT 11 (10.6%) females in IPT group and 35(35%) in control group remained depressed. Moreover, Mann-Whitney test showed the intervention group mean was lesser than control group mean (33.03<77.97) with highly significant of results p<0.001. These findings align with the study in respect to decrease level of depression after getting IPT and found it highly effective to reduce the level of depression among postpartum females.22
Thus, according to our data there was significant difference seen regarding decrease symptoms of depression in intervention group as compared to control group, depressed mood p<0.001, CI (0.000,0.027), feeling of guilt p<0.001, CI (0.000, 0.027) and insomnia p<0.007, CI (0.000,0.043) showed highly significant results. According to a comprehensive systematic review and meta-analysis encompassing 40 selected articles, an examination was conducted to compare the efficacy of IPT against control groups. The outcomes revealed statistically significant difference between the IPT and control group (p < 0.0001), thereby affirming its utility in the management of major depressive disorder, postpartum depression and particularly among Chinese first-time mothers.23 Furthermore, an additional meta-analysis lent further credence to the effectiveness of IPT in amending depressive symptoms among postpartum females.24
Furthermore, according to our study before and after intervention results showed highly significant of results in intervention group, depressed mood p<0.001, CI (0.000, 0.020), suicide p<0.931, CI (0.98, 1.00), insomnia early, mid-night and early morning p<0.001, CI (0.000, 0.020). A qualitative study found IPT an acceptable treatment for the first time parents to facilitate the healthy transition into parenthood.25 Moreover, another study showed similar findings that IPT may be effective to decrease depression level and help in role adaption.26 Likewise, a study found IPT more effective in treating symptoms of PPD as compared to treatment as usual (TAU).27
Concurrently, at the termination phase participants were asked about review of IPT, 80 out of 110 participants (72%) were satisfied that IPT was very beneficial to them. According to case presentation of 38 years old married female with major depressive disorder one month after the birth of her child. She was battling an internal conflict of continuing to pursue her career as an obstetrician and fulfilling her responsibility as a wife and a mother. After getting eight sessions of IPT, the patient reported improvement in depressive symptoms and relationship with her husband. She felt more confident to start doing clinical work and found IPT very effective.10
Strength of Study
Our trial has multiple strengths, RCT used as study design. Moreover, single blinding helped to minimize the selection and assessment bias. Additionally, research context was tertiary care hospital Lahore with facilities of well-known psychologist and psychiatric department. IPT was given under supervision of expert clinical psychologist and the participants who were diagnosed as severe depression refer to the psychiatric department of the same tertiary care hospital. Another strength was provision of supplementary material like intervention booklet and videos to the participants at the termination of therapy for relapse prevention.
Limitation of Study
Despite the strengths, there were some limitations of study. Only one variable of IPT studied role transition not others discussed, interpersonal conflict, interpersonal deficit and grief. We specifically studied the challenges females face while adopting new role (being mother) that may lead to PPD and introduced healthy ways to adopt new role positively and avoid from PPD. While other variables discuss the conflicts between husband and wife, response of females on preterm birth or still birth and have some personality traits that do not maintain existing relationship or build new one. Due to limited resources, it could not be possible to study two or three variables at once, but it may be beneficial to explore other factors contributing to PPD and mitigate their risk of occurrence.
Moreover, one study setting has selected for data collection, data was not collected from all four provinces of Pakistan. However, females in different provinces have common challenges related to role transition (being new parent). Reason to select one study setting was financial constraints, researcher was not facilitated by funds for research from parent institutes not from government agencies.
Another limitation was potential for recall bias due to data being reliant on participant responses. Patients were not sure about some questions such as weight of patient, anxiety, and somatic symptoms so it would be better to corroborate responses with other data sources such as files and medical record of participants.
Additionally, during intervention relapse was prevented but there is a potential of relapse after termination of therapy. However, long term follow-up studies can mitigate this issue where patient would be allowed to get in touch with therapist and take guidance even after termination of therapy to deal with stressors of their daily routine.
Finally, no any strategy proposed for potential real-life stressors, if participants may expose to any stressor like death of family member, divorce or loss of a baby would trigger a potential relapse of depression. However, real life challenges could not be avoided but strong social support of loved ones may be helpful to avoid from severe mental illness.
Recommendations
It is recommended for future studies to conduct on large data set from all over the Pakistan. Actual as well as potential factors contributing to PPD should be explored. Strong strategies should be implemented for relapse prevention. Moreover, beside the physical health government should focus on the mental health of people and enhance awareness regarding symptoms of PPD and introduce healthy ways for its prevention. Additionally, more research is required to assess the effectiveness of early screening (specifically within 10 days of postpartum), and intervention using IPT for PPD.
Conclusion
The results indicate a concerning prevalence rate of PPD among the study sample with many cases remaining undiagnosed and untreated. More positively, the study demonstrates the potential of IPT as an effective method to mitigate mild to moderate PPD. This research suggests the incorporation of IPT into therapeutic models could result in timely, potentially preventive interventions and lessen the occurrence of severe complications.
Practical Implication
The result of this study supports the use of IPT to treat the PPD and avoid severe mental disorders like psychosis and schizophrenia. Moreover, healthy mothers can care their babies in better way. Additionally, IPT will be cost effective to whom can’t afford pharmacological treatment of depression and has no harm for the mothers and lactation exposure to the babies.
Acknowledgement
Mr. Adnan Yaqoob helped in formatting the synopsis and to obtain the ethical approval from respective organization.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial and not for profit sectors.
Conflict of Interest
There are no relevant conflicts of interest to disclose.
Authorship Contribution
Concept, Material, Data collection, Intervention, Data Analysis, Thesis Write up Arshad. S., Supervision, Critical Review Afzal. M., Supervision Sarwar. H.
References
- Wubetu AD, NA Engidaw, KD Gizachew. Prevalence of postpartum depression and associated factors among postnatal care attendees in Debre Berhan, Ethiopia, 2018. BMC Pregnancy Childbirth. 2020; 20(1): 189. DOI: 10.1186/s12884-020-02873-4
- Akram B, Ahmed MA, Maqsood F, et al. Postpartum depression and suicidal ideation in new mothers with hearing loss: Perceived social support as a moderator, a multicentre study. J Pak Med Assoc. 2020; 70: 213-8. DOI: https://pubmed.ncbi.nlm.nih.gov/32063609/
- Keepanasseril A, Singh S, Bharadwaj B. Postpartum mental health status & role transition to mother in primigravid women: A cross-sectional study. Journal of Reproductive and Infant Psychology. 2021; 1-10. DOI: https://pubmed.ncbi.nlm.nih.gov/34338099/
- Wang Z, Liu J, Shuai H, et al. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. 2021; 11(1): 543. DOI: 10.1038/s41398-021-01663-6
- Yadav T, Shams R, Khan AF, et al. Postpartum Depression: Prevalence and Associated Risk Factors Among Women in Sindh, Pakistan. Cureus. 2020; 12(12): e12216. DOI: https://ncbi.nlm.nih.gov/pmc/articles/PMC7815271/
- Abdelmola AO, Bahari A, Gosadi I, et al. Prevalence and Factors Associated with Maternal Postpartum Depression among Mothers in Saudi Arabia: A Cross-Sectional Study. in Healthcare. 2023. DOI: https://pubmed.ncbi.nlm.nih.gov/36766918/
- Kang HK, John D, Bisht B, et al. PROTOCOL: Effectiveness of interpersonal psychotherapy in comparison to other psychological and pharmacological interventions for reducing depressive symptoms in women diagnosed with postpartum depression in low and middle-income countries: A systematic review. Campbell Systematic Reviews, 2020; 16(1): e1074. DOI: https://pubmed.ncbi.nlm.nih.gov/37131982/
- Agrawal I, Mehendale AM, Malhotra R. Malhotra, Risk factors of postpartum depression. Cureus. 2022; 14(10): e30898. DOI: https://pubmed.ncbi.nlm.nih.gov/36465774/
- Xiao L. Agomelatine for postpartum depression and breastfeeding. Therapeutic Advances in Psychopharmacology. 2021; 11: 20451253211022172. DOI: https://ncbi.nlm.nih.gov/pmc/articles/PMC8182171/
- Tan HJR. An Illustration of Interpersonal Psychotherapy for Perinatal Depression. Case Rep Psychiatry. 2020. DOI: 10.1155/2020/8820849
- Rajhans P, Hans G, Kumar V, et al., Interpersonal Psychotherapy for Patients with Mental Disorders. Indian journal of psychiatry. 2020; 62(Suppl 2): S201. DOI: https://ncbi.nlm.nih.gov/pmc/articles/PMC7001362/
- Stewart DE, Vigod SN. Postpartum Depression: Pathophysiology, Treatment, and Emerging Therapeutics. Annu Rev Med. 2019; 70: 183-196. DOI: 10.1146/annurev-med-041217-011106
- Rhattigan Y. The efficacy of interpersonal therapy as a psychotherapeutic intervention in the treatment of postpartum depression. 2020. DOI: https://esource.dbs.ie/items/
9c89e7a1-5f81-439f-b191- b546a3308e99 - Moustafa AA, Crouse JJ, Herzallah MM, et al. Depression Following Major Life Transitions in Women: A Review and Theory. Psychol Rep. 2020; 123(5): 1501-1517. DOI: 10.1177/0033294119872209
- O'Hara MW, McCabe JE. Postpartum depression: current status and future directions. Annual review of clinical psychology. 2013; 9: 379-407. DOI: https://pubmed.ncbi.nlm.nih.gov/23394227/
- Hashmi AM, Naz S, Asif A, et al. Urdu translation of the Hamilton Rating Scale for Depression: Results of a validation study. Pak J Med Sci. 2016; 32(6): 1479-1483. DOI: 10.12669/pjms.326.11399
- Abenova M, Myssayev A, Kanya L, et al. Prevalence of postpartum depression and its associated factors within a year after birth in Semey, Kazakhstan: A cross sectional study. Clinical Epidemiology and Global Health. 2022; 16: 101103. DOI: https://sciencedirect.com/science/article/pii/S2213398422001452
- Wang Z, Liu J, Shuai H, et al. Mapping global prevalence of depression among postpartum women. Translational psychiatry. 2021; 11(1): 543. DOI: https://pubmed.ncbi.nlm.nih.
gov/34930896/ - Zejnullahu VA, Ukella-Lleshi D, Zejnullahu VA, et al. Prevalence of postpartum depression at the clinic for obstetrics and gynecology in Kosovo teaching hospital: Demographic, obstetric and psychosocial risk factors. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2021; 256: 215-220. DOI: https://pubmed.ncbi.nlm.nih.gov/33248376/
- Nakamura Y, Okada T, Morikawa M et al. Perinatal depression and anxiety of primipara is higher than that of multipara in Japanese women. Sci Rep. 2020; 10(1): 17060. DOI: https://nature.com/articles/s41598-020-74088-8
- Zhang L, Wang L, Yuan Q, et al. The mediating role of prenatal depression in adult attachment and maternal-fetal attachment in primigravida in the third trimester. BMC Pregnancy Childbirth. 2021; 21(1): 307. DOI: 10.1186/s12884-021-03779-5
- Dennis CL, Grigoriadis S, Zupancic J, et al. Telephone-based nurse-delivered interpersonal psychotherapy for postpartum depression: nationwide randomised controlled trial. The British Journal of Psychiatry. 2020; 216(4): 189-196. DOI: https://pubmed.ncbi.nlm.nih.gov/32029010/
- Zheng W, Tang L, Xu F, et al. Efficacy of interpersonal psychotherapy in mainland China: a systematic review and meta-analysis. Frontiers in Psychiatry. 2023; 14(1): 1160081. DOI: https://doi.org/10.3389/fpsyt.2023.1160081
- Bright KS, Charrois EM, Mughal MK, et al. Interpersonal psychotherapy for perinatal women: a systematic review and meta-analysis protocol. Systematic reviews. 2019; 8(1): 248. DOI: https://
systematicreviewsjournal. biomedcentral.com/articles/10. 1186/s13643-019-1158-6 - Ngai FW, Lam W. Couple-based interpersonal psychotherapy for first-time parents: A process evaluation. Journal of Pediatric Nursing. 2023. DOI: https://pubmed.ncbi.nlm.nih.
gov/37385939/ - Pouyan F, Akbari Kamrani M, Rahimzadeh M, et al. Effect of interpersonal psychotherapy oriented child birth education on stress and role adaptation in mothers with premature birth: a randomized clinical trial. Iranian Journal of Psychiatry and Behavioral Sciences. 2019; 13(1): e86645. DOI: https://brieflands.com/articles/ijpbs-86645
- Schramm E, Mack S, Thiel N, et al. Interpersonal Psychotherapy vs. Treatment as Usual for Major Depression Related to Work Stress: A Pilot Randomized Controlled Study. Front Psychiatry. 2020; 11: 193. DOI: 10.3389/fpsyt.2020.00193
- Alhusaini NA, Zarban NA, Shoukry ST, et al. Prevalence of Postpartum Depression Among Mothers Giving Birth at King Abdulaziz University Hospital, Jeddah, Kingdom of Saudi Arabia From 2020 Until 2022. Cureus. 2022; 14(11): e31365. DOI: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9741841/