
Does Mental Health impact the outcomes of Total Ankle Arthroplasty? A Systematic Review
Margaret A. Sinkler1*, Amir H. Karimi2, Mohamed E. El-Abtah2, John E. Feighan1, Ethan R. Harlow1, Heather A. Vallier2
1University Hospitals, Case Western Reserve University, Cleveland, OH, USA
2Case Western Reserve University School of Medicine, Cleveland, OH, USA
Abstract
Studies have demonstrated that depression, anxiety, negative mood, and pain catastrophizing influence outcomes following total hip, knee, and shoulder arthroplasty thus providing evidence-based counseling on expected postoperative outcomes. The purpose of this review is to establish the prevalence of mental health conditions, impact of mental health conditions on patient-reported outcome measures, and the impact on length of stay and discharge disposition in patients undergoing total ankle arthroplasty (TAA). An online search utilizing the Cochrane Central Register of Controlled Trials, PubMed, Google Scholar, and CINAHL databases was performed to identify relevant articles published between 2010 and 2022. Seven studies were included in the systematic review. Depression was the most common mental health comorbidity with a pooled prevalence of 12.9%. Mental health comorbidities were associated with inferior patient reported outcomes measures. Additionally, depression was a pre-operative predictive factor in poor outcomes when utilizing the PROMIS score. The presence of a mental health comorbidity demonstrated an increased risk of nonhome discharge, length of stay, complication rate, infection, and narcotic use. Psychiatric comorbidities, particularly depression, were predictors of negative postoperative outcomes. This review reinforces the significant impact of mental health disorders and psychiatric comorbidities on clinical outcomes following TAA.
Level of Evidence: Level III
Introduction
Ankle osteoarthritis (OA) is a major cause of disability with an incidence of 47.7 per 100,000 thus affecting 1% of the world population1,2. Ankle OA has been shown to have a similar impact on mental and physical disability compared to end-stage heart failure and hip arthritis3,4. The two main surgical treatments include ankle arthrodesis and total ankle arthroplasty (TAA). Historically, ankle arthrodesis was the treatment of choice for ankle OA but it may lead to inferior functional outcomes compared to arthroplasty and may hasten adjacent joint degeneration. The popularity of TAA as a viable treatment strategy for ankle OA is increasing as it mitigates some of the negative functional consequences associated with arthrodesis while also achieving similarly excellent pain relief. While early generations of TAA implants had poor clinical results and high rates of aseptic loosening, recently reported intermediate and long term outcomes have suggested that TAA is comparable in regard to complication and revision rates5,6.
While a prior systematic review demonstrated that age, obesity, arthritis etiology, surgeon experience, surgical technique, and prosthesis design have all impact outcomes of TAA7,8, they did not include the potential impact of mental health and psychological factors on clinical outcomes. Many studies have revealed associations between psychiatric comorbidities and increased risks of negative treatment outcomes in other orthopedic procedures, particularly when performed for degenerative conditions like osteoarthritis9-11. A variety of studies have demonstrated that depression, anxiety, negative mood, and pain catastrophizing influence postoperative outcomes following total hip, knee, and shoulder arthroplasty12-16. The presence of these mental and psychological factors has been shown to lead to persistent pain, reduced level of function, decreased overall satisfaction, and longer hospital stay17-19. Unlike the aforementioned arthroplasty procedures, a formal review has not been conducted to generate a holistic understanding of the impact of mental health on patients undergoing TAA. Therefore, the purpose of this systematic review is to determine the association between mental health disorders and the outcome following TAA.
Methods
Search Strategy and Criteria
An electronic search was conducted in July 2022 in accordance to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) checklist to establish relevant studies for inclusion in the review using the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Google Scholar, and CINAHL databases. All the articles relevant to the subject of interest were retrieved using the search strategy as detailed. The search involved the use medical subject headings (MeSH) in combination with keywords and free words ("Mental Disorders"[Mesh] OR "Mental Health"[Mesh] OR "Psychotropic Drugs"[Mesh] OR "Anxiety"[Mesh] OR "mental illness" OR "psychiatric" OR "anxiety" OR "psychiatric") AND ("ankle arthroplasty" OR "ankle replacement"). A manual hand search was also done on the references of eligible articles for other relevant journal materials.
Inclusion and Exclusion
For inclusion in this systematic review, each study met the following criteria: (1) an accepted and published scholarly article, (2) included patients who underwent total ankle arthroplasty, (3) reported mental health disorders or psychiatric comorbidities, (4) reported ankle-specific preoperative and postoperative measurements, (5) were written in the English language, (6) full text availability, and (7) published between 2010 to 2022.
The exclusion criteria consisted of (1) no reported surgical outcomes, (2) studies discussing animal-related experiments, (3) publications in non-peer reviewed journals, (4) case reports, case series, and letters to editors.
Assessment of Study Quality
The quality of included studies was independently evaluated by the two reviewers (A.K and M.E) using the Methodological Index for Nonrandomized Studies (MINORS) tool20. The MINORS tool grades non-comparative studies on a scale from 0 to 16 based on eight criteria domains relating to the article design, outcomes evaluated, and follow-up. Each criteria within the MINORS tools was scored 0 if not reported, 1 when reported and not clear or adequate, and 2 when adequately reported. Level of evidence was assigned based on the methodology and validity of the study designed21.
Data Collection and Abstraction
Following the initial search query, the eligibility of each of the retrieved articles was independently assessed by two investigators (A.K. and M.E.). A total of 1286 titles were identified via databases with an additional 3 identified via manual hand search on the references of included studies. All the abstracts and titles of the retrieved studies (n=1289) were analyzed for relevance by each investigator. Disagreements were discussed, and a third independent reviewer (M.S.) was consulted to achieve consensus. After the first screening and removal of duplicates, the full-texts of the resulting studies (n=49) were analyzed. All the studies that were not eligible were excluded (n=42). The systematic inquiry resulted in seven articles included in the study.
Data extraction was independently performed by the two authors for the selected articles and the following information was extracted from the selected articles: name of authors and year of publication, study design, sample size, age, mental health disorders/comorbidities, covariates or controlled variables, results expressed on statistical effect size, conclusion, and inference. Any discrepancy was reviewed by a third author for accuracy.
Results
A total of 1289 studies were generated through the search process. After duplicate removal and screening via titles, abstract, and full-text, seven studies fully met the inclusion criteria and were thus included in the analysis for this systematic review (Figure 1). All the necessary data were retrieved from the studies that ascertained the correlation between mental health disorders and post-operative outcomes and complications. Three of the included studies were prospective studies22-24 and the other four were retrospective studies25-28. The level of evidence (II and III) was reported for the included studies. The studies scored an average of 15.14 ± 0.69 on the MINORS scale (Table 1).
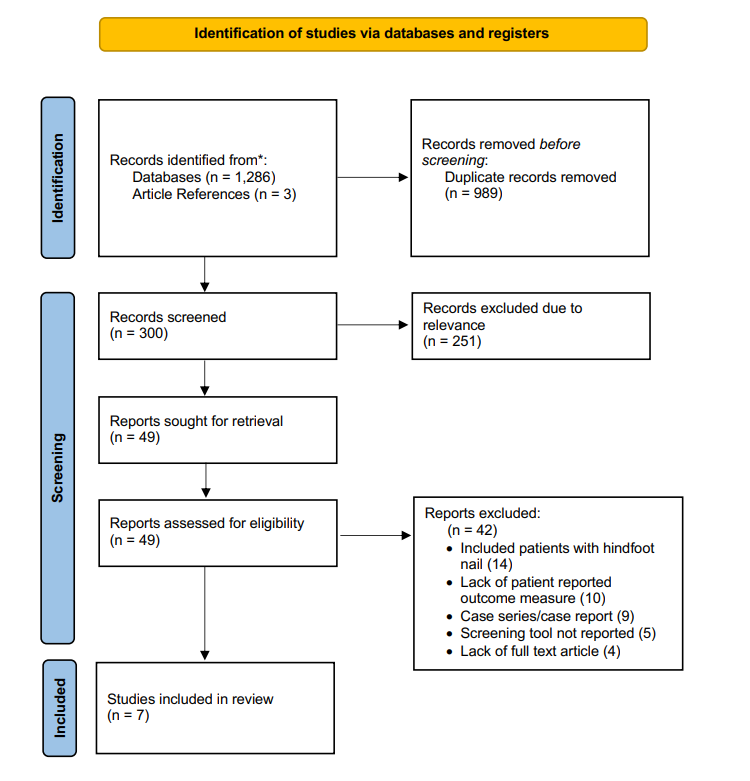
Figure 1: PRISMA Flow Diagram
Table 1: Individual MINORS Score of each Included Studies
|
Author |
C1 |
C2 |
C3 |
C4 |
C5 |
C6 |
C7 |
C8 |
C9 |
C10 |
C11 |
C12 |
Total |
|
Conti et al.24 |
2 |
2 |
2 |
1 |
2 |
2 |
1 |
2 |
2 |
NA |
NA |
NA |
16 |
|
Cunningham et al.22 |
2 |
2 |
2 |
1 |
2 |
2 |
1 |
1 |
2 |
NA |
NA |
NA |
15 |
|
Cunningham et al.23 |
2 |
2 |
2 |
1 |
1 |
2 |
1 |
1 |
2 |
NA |
NA |
NA |
14 |
|
Kim et al.26 |
2 |
2 |
2 |
2 |
1 |
2 |
1 |
2 |
2 |
NA |
NA |
NA |
16 |
|
Mulligan et al.28 |
2 |
2 |
2 |
1 |
1 |
2 |
1 |
1 |
2 |
NA |
NA |
NA |
14 |
|
Steele et al.27 |
2 |
2 |
2 |
1 |
1 |
2 |
1 |
1 |
2 |
NA |
NA |
NA |
15 |
|
Wilson et al.25 |
2 |
2 |
2 |
2 |
1 |
2 |
1 |
2 |
2 |
NA |
NA |
NA |
16 |
C1: a clearly stated aim; C2: inclusion of consecutive patients; C3: prospective collection of data: C4: endpoint appropriate to the aim of the study; C5: unbiased assessment of the study endpoint; C6: follow up appropriate to the aim of the study; C7: loss of follow up less than 5%; C8: prospective calculation of the study size; C9: an adequate control group; C10: contemporary group; C11: baseline equivalent of groups; C12: adequate statistical analysis
Mental health conditions included within the articles were depression22-28, schizophrenia28, bipolar disorder28 and overall mental health27. The prevalence of depression ranged from 11.4-32.5%22-25 (Table 2). Depression was either defined by a patient-reported outcome measure including the Patient-Reported Outcomes Measurement Information System (PROMIS) score24, Center for Epidemiologic Studies Depression scale (CES-D)26, the Patient Health Questionnaire (PHQ-9)26, clinical intake form28; or the International Classification of Disease code (ICD-9-CM and ICD-10)22,23,25. Pooling the rates of depression across the four studies resulted in an overall prevalence of 12.9%. Mulligan et al. grouped depression, schizophrenia, and bipolar disorder together designated as mood disorders identified on a patient intake questionnaire. There was a 28% prevalence of mood disorders within their cohort28.
Table 2: Characteristics of Included Studies and Prevalence of Mental Health Illnesses
|
Author Name |
Year |
Level of Evidence |
Study Design |
Sample size |
Mental health illness |
Diagnosis Method |
Prevalence |
|
Conti et al.24 |
2021 |
III |
Retrospective cohort |
105 patients |
Depression |
PROMIS Scores |
- |
|
Cunningham et al.22 |
2019 |
IV |
Prospective cohort |
668 patients |
Depression |
ICD-9-CM and ICD-10 Codes |
22.2% |
|
Cunningham et al.23 |
2021 |
III |
Prospective cohort |
612 patients |
Depression |
ICD-9-CM and ICD-10 Codes |
21.1% |
|
Kim et al.26 |
2020 |
III |
Retrospective cohort |
40 patients |
Depression |
CES-D and PHQ-9 Scores |
32.5% |
|
Mulligan et al.28 |
2016 |
III |
Retrospective cohort |
132 patients |
Mood disorders (depression, bipolar and schizophrenia) |
Intake questionnaire |
28% |
|
Steele et al.27 |
2020 |
III |
Retrospective cohort |
491 patients |
Overall Mental Health |
SF-36 MCS |
- |
|
Wilson et al.25 |
2020 |
III |
Retrospective cohort |
8047 patients |
Depression |
ICD-9-CM and ICD-10 Codes |
11.4% |
ICD = International Classification of Diseases; PROMIS patient reported outcome measurement information system; CES-D = Center of Epidemiologic Studies Depression Scale; PHQ-9 = Patient Health Questionnaire; SF-36 = short form – 36; MCS = mental component score
Five of the seven studies evaluated the impact of mental health comorbidities using patient-reported outcomes measures (PROMs) utilizing PROMIS, Short Musculoskeletal Functional Assessment (SMFA), 36-item Short Form (SF-36), Visual Analog Scale (VAS), and American Orthopaedic Foot and Ankle Score (AOFAS)22-24,26,28 (Table 3). Cunningham et al. demonstrated that patients with depression had significantly smaller improvements at both 2- and 5-year follow-up22,23. Kim et al. showed that postoperative VAS scores (3.1 vs 1.4, p < 0.01) were inferior in the cohort with depression compared to the cohort without; additionally the AOFAS scores (89.3 vs 95 p <0.001) were worse in the depression cohort26. Similarly, Mulligan et al. demonstrated that mood disorder was a risk factor for increased VAS score at follow-up (p<0.001)28. When utilizing depression scores as a pre-operative predictor, Conti et al. found that lower PROMIS depression t scores (less than 43.3 with a 95% sensitivity threshold, 95% CI = 0.041 – 0.649, p<0.001) were predictive in achieving the minimal clinically important difference post-operatively. The posttest probability of achieving the minimal clinically important difference (MCID) with a score less than 43.3 was only 8.8%24. Steele et al. showed that those with a higher SF-36 MCS score where more likely to achieve MCID in Short Musculoskeletal Function Assessment score compared to those with lower SF-36 MCS score (P = 0.005)27.
Table 3: The Impact of Mental Health Illnesses on Outcomes of TAA
|
Author Name |
PROM Measured |
PROM Outcome |
Clinical Variables |
Clinical Outcome |
Conclusion |
|
Conti et al.24 |
PROMIS Depression t Score |
Patients with a pre-operative PROMIS scores under 43.3 are predicted to reach MCID using a 95% sensitivity threshold |
- |
- |
The pre-operative PROMIS depression scores depression could be used to predict postoperative clinical outcomes after surgery. |
|
Cunningham et al.22 |
SMFA Function, SMFA Bother, SF-36 PCS, SF-36 MCS, and VAS |
Depression was significantly associated with smaller improvements in all outcomes at both 2- and 5-year follow up (p < 0.05) |
- |
- |
Patients experienced inferior outcomes on overall improvement and increased risk of pain. Depression was reported to potentially modifiable risk factor. |
|
Cunningham et al.23 |
SMFA Function, SMFA Bother, SF-36 PCS, SF-36 MCS, and VAS |
Patient with depression had less improvement in physical functioning (51.2 vs.75.2, p<0.001) and pain scores (9 vs. 4, p<0.001) |
- |
- |
Depression and diminishing preoperative mental health status increased the risks of experiencing smaller postoperative improvement. |
|
Kim et al.26 |
AOFAS and VAS |
Depressed group showed worse outcomes across the postoperative AOFAS and VAS than the non-depressive group (89.3 vs 95 p <0.001; 3.1 vs 1.4, p < 0.01) |
- |
- |
The clinical outcome after TAA was poorer in depressive than non-depressed group, implying that depressive symptoms were predicative factors for less improvements in clinical outcomes after surgery. |
|
Mulligan et al.28 |
VAS |
Mood disorder was a risk factor for increased VAS (P < .01). |
Narcotic use past 90 days |
Mood disorder (P < .01) was a risk factor for continued narcotic use along with pre-operative narcotic use (P < .01) and chronic pain (P = .02), |
Patients who experienced increased postoperative chronic pain were diagnosed with mood disorder as well as use of narcotics and tobacco preoperatively. |
|
Steele et al.27 |
- |
- |
MCID after 2 years |
Higher SF-36 MCS scores achieved were more likely to achieve MCID after 2 years (P = 0.005) |
Higher baseline SF-36 MCS score was associated with increased improvement in Short Musculoskeletal Function Assessment function scores |
|
Wilson et al.25 |
- |
- |
Non-home discharge, extended LOS, wound complication, prosthetic complications, joint infection, superficial infection and medical complications |
Increased rates of non-home discharge (OR 1.61, P<0.001), extended LOS (>2 days; OR 1.34, P<0.001), prosthetic complication (OR 1.39, P=0.005), wound complication (OR 1.59, P=0.012), prosthetic joint infection (OR 1.82, P=0.031), superficial infection (OR 1.62, P=0.041), and medical complication (OR 1.32, P=0.026) |
Depression was common for TAA patients and was associated with increased healthcare utilization and complications after surgery. |
PROM = patient reported outcome measures; PROMIS patient reported outcome measurement information system; SMFA = short musculoskeletal function assessment; SF-36 = short form – 36; MCS = mental component score; PCS = physical component score; VAS = visual analog scale; AOFAS = American Orthopedic Foot and Ankle Score; OR = odds ratio; and CI = confidence interval; MCID = minimal clinically important difference
Two studies evaluated the association between mental health and hospital courses. Wilson and colleagues found that patients with diagnosed depression had an increased risk of non-home discharge (OR 1.61), extended length of hospital stay (OR 1.34), development of prosthetic complications (OR 1.39), wound complications (OR 1.59), prosthetic joint infection (OR 1.82), superficial infection (OR 1.62), and medical complication (OR 1.62)25. Mulligan et al. found mood disorders; which included depression, schizophrenia, and bipolar disorder, as a risk for continued narcotic use past 90 days (p<0.01)28. In summary, the findings from the above studies reported evidence of an association of various psychiatric comorbidities on post-operative discharge destination and complications and following TAA.
Discussion
With the increasing rate of total ankle arthroplasty (TAA) being performed6,29, the identification of procedurally specific risk factors is paramount. Although established in other arthroscopy procedures, there are only a few studies discussing the role of mental health with outcomes of TAA. Our review identified seven studies which address the prevalence, impact on patient reported outcome measures, and hospital course and discharge disposition of patients undergoing TAA with respect to mental health. The mental health disorders that were identified with the highest prevalence in this patient population included depression, schizophrenia, and bipolar disorder. Mental health was found to impact rates of surgical site infection, pain, functional status, prosthetic complications, length of hospital stay, non-home discharge, wound infection, and periprosthetic joint infection. Overall, this review strongly suggests that there is an association between mental health disorders and psychiatric comorbidities with negative clinical outcomes following TAA.
Our review found that the prevalence of depression ranged from 11.4-32.5% with an overall pooled rate of 12.9%. A single study found a prevalence of mood disorders, including depression, schizophrenia, and bipolar disorder, of 28%. From 2013-2016, 8.1% of American adults over the age of 20 reported at least a two week period of depression31. Additionally, in 2020, 21% of American adults were diagnosed with a mental illness32. Similarly to the TAA cohort, increased rates of depression are also reported in patients undergoing hip and knee arthroplasty11,33. The increased rates of mental health illnesses in the patients undergoing TAA are likely due to the poorer mental and physical quality of life experienced by patients with ankle osteoarthritis with rates of depression in studies evaluating chronic foot and ankle disease and Charcot foot reported between 27%-42%9,34,35. There is a substantial range of depression rates across the studies included in this review which may be explained by the heterogeneity of the method of identifying depression in each cohort. As studies have demonstrated that point of care depression screens has a higher sensitivity compared to diagnosis codes9, our pooled number is likely negatively skewed as a majority of the cohort was collected using diagnosis codes. The available literature utilizes depression most frequently whereas only one study captured additional mental illnesses including bipolar disorder and schizophrenia. Improved preoperative identification of mental illness and investigation is needed to understand the nuances of these additional diagnoses.
Depression was associated with inferior outcomes across both function and pain-based patient reported outcomes measures in addition to being a predictor of achieving a postoperative minimal clinically important difference22-26. Mood disorders consisting of depression, schizophrenia, and bipolar disorders showed increased pain scores at follow up28. While there is a well-known interaction between psychological comorbidities and musculoskeletal pain, the relationship is quite nuanced and poorly understood36,37. Patients' functional outcomes following TAA are known to be improved with proper physical therapy38. Of note, mental health disorders are known to affect a patient’s rehabilitation and impact their overall lifestyle, potentially explaining one aspect of the observed poor surgical outcomes39-41. As patient expectations are becoming an increasingly recognized predictor of postoperative outcomes42, pre-operative mental health screenings should play a role in setting these expectations. As Conti et al. demonstrated, collecting PROMIS scores help predict who will reach a perceived improved outcome and would assist in framing the discussion24.
The two studies demonstrated that mental health comorbidities were associated with increased complication rates, length of hospital stay, and narcotic usage in patients undergoing TAA. Similar trends have been observed in patients undergoing total knee and hip procedures including increased medical complications10,11, prosthetic joint infection10, and length of stay43. Outside of arthroplasty patients, medically admitted patients with depression also experience prolonged length of stay44. One rationale may relate to the heightened pain scores seen in patients with depression leading to a longer length of stay. When evaluating the increased infection rates, psychological distress in humans has been correlated with a systemic low grade inflammatory state which could potentially exhaust immune systems increasing susceptibility to local infection45,46. Of note, the findings of this review should be interpreted carefully as they are drawn from two isolated studies. The relationship between the outcomes and mental health is likely complex, indirect, and derived from mood-physiology interactions. With arthroplasty transitioning towards outpatient procedures based on patient selection, further quantifying the role of mental health comorbidities with complication rate should occur.
While this review has suggested that patients with a preoperative diagnosis of depression are at an increased risk of poor outcomes following TAA, it should not serve as a contraindication. While depressed patients may not experience an equivocal level of improvement, they benefit from the procedure addressing their underlying pathology. Patients would likely benefit from additional counseling regarding their expected recovery, residual symptoms, pain, and functional improvement following their TAA. Future efforts should focus on incorporating mental health into risk-adjustment models to compare with other known negative predictors of TAA. Additionally, a preoperative diagnosis of depression may be a modifiable risk factor. Patients will likely experience improved post-operative outcomes through the use of a multidisciplinary strategy that addresses both musculoskeletal pathology and mental health. Future studies are needed to assess the impact of diagnosis and subsequent treatment of mental health surrounding TAA.
The present systematic review should be considered in light of its limitations. First and foremost, the study is limited as a result of the small number of articles included that assessed the study objective; hence, the conclusions presented are preliminary and require additional studies for confirmation. The articles had substantial heterogeneity precluding pooling for a meta-analysis. Across many of the studies, mental health illnesses were diagnosed using self-reporting methods rather than a formal assessment potentially affecting the accuracy of diagnosis. Additionally, the studies did not provide information regarding if patients received any treatment for their mental health conditions before undergoing TAA. Only one study presented an odds ratio derived from a multivariate regression. Thus, the interplay between mental health and other coexisting medical comorbidities requires further investigation. The articles included retrospective and prospective observational cohorts with the potential for selection bias by the study investigator or participants30. When performing our review, we strove to limit bias using an a priori protocol with detailed inclusion criteria for article selection and data extraction.
Conclusion
Mental health illnesses have an impact on the outcomes of total ankle arthroplasty. Due to the increasing popularity of the surgical procedure and the prevalence of mental illness, understanding the role of mental health on patient outcomes has implications for patient education, experience, and selection. Mental health illnesses, especially depression, have been correlated to decreased patient reported outcomes measures, higher complication rates, increased length of hospital stay, and increased narcotic usage. Thus, we advocate for routine mental health screening during the pre-operative assessment before total ankle arthroplasty.
References
- Goldberg AJ, MacGregor A, Dawson J, et al. The demand incidence of symptomatic ankle osteoarthritis presenting to foot & ankle surgeons in the United Kingdom. The Foot. 2012; 22(3): 163-166. doi:10.1016/J.FOOT.2012.02.005
- Barg A, Pagenstert GI, Hügle T, et al. Ankle osteoarthritis: etiology, diagnostics, and classification. Foot Ankle Clin. 2013; 18(3): 411-426. doi:10.1016/j.fcl.2013.06.001
- Saltzman CL, Zimmerman MB, O’Rourke M, et al. Impact of comorbidities on the measurement of health in patients with ankle osteoarthritis. J Bone Joint Surg Am. 2006; 88(11): 2366-2372. doi:10.2106/JBJS.F.00295
- Glazebrook M, Daniels T, Younger A, et al. Comparison of health-related quality of life between patients with end-stage ankle and hip arthrosis. J Bone Joint Surg Am. 2008; 90(3): 499-505. doi:10.2106/JBJS.F.01299
- Haddad SL, Coetzee JC, Estok R, et al. Intermediate and long-term outcomes of total ankle arthroplasty and ankle arthrodesis. A systematic review of the literature. J Bone Joint Surg Am. 2007; 89(9): 1899-1905. doi:10.2106/JBJS.F.01149
- Lawton CD, Prescott A, Butler BA, et al. Modern total ankle arthroplasty versus ankle arthrodesis: A systematic review and meta-analysis. Orthop Rev (Pavia). 2020; 12(3): 8279. doi:10.4081/or.2020.8279
- Zhao D, Huang D, Zhang G, et al. Positive and negative factors for the treatment outcomes following total ankle arthroplasty? A systematic review. Foot Ankle Surg. 2020; 26(1): 1-13. doi:10.1016/j.fas.2018.12.003
- Sansosti LE, Van JC, Meyr AJ. Effect of Obesity on Total Ankle Arthroplasty: A Systematic Review of Postoperative Complications Requiring Surgical Revision. J Foot Ankle Surg. 2018; 57(2): 353-356. doi:10.1053/j.jfas.2017.10.034
- Nakagawa R, Yamaguchi S, Kimura S, et al. Association of Anxiety and Depression With Pain and Quality of Life in Patients With Chronic Foot and Ankle Diseases. Foot Ankle Int. 2017; 38(11): 1192-1198. doi:10.1177/1071100717723133
- Klement MR, Nickel BT, Penrose CT, et al. Psychiatric disorders increase complication rate after primary total knee arthroplasty. Knee. 2016; 23(5): 883-886. doi:10.1016/j.knee.2016.05.007
- Browne JA, Sandberg BF, D’Apuzzo MR, et al. Depression is associated with early postoperative outcomes following total joint arthroplasty: a nationwide database study. J Arthroplasty. 2014; 29(3): 481-483. doi:10.1016/j.arth.2013.08.025
- Vajapey SP, Cvetanovich GL, Bishop JY, et al. Psychosocial factors affecting outcomes after shoulder arthroplasty: a systematic review. J Shoulder Elbow Surg. 2020; 29(5): e175-e184. doi:10.1016/j.jse.2019.09.043
- Buirs LD, van Beers LWAH, Scholtes VAB, et al. Predictors of physical functioning after total hip arthroplasty: a systematic review. BMJ Open. 2016; 6(9): e010725. doi:10.1136/bmjopen-2015-010725
- Lingard EA, Katz JN, Wright EA, et al. Predicting the outcome of total knee arthroplasty. J Bone Joint Surg Am. 2004; 86(10): 2179-2186. doi:10.2106/00004623-200410000-00008
- Gandhi R, Dhotar H, Razak F, et al. Predicting the longer term outcomes of total knee arthroplasty. Knee. 2010; 17(1): 15-18. doi:10.1016/j.knee.2009.06.003
- Vissers MM, Bussmann JB, Verhaar JAN, et al. Psychological factors affecting the outcome of total hip and knee arthroplasty: a systematic review. Semin Arthritis Rheum. 2012; 41(4): 576-588. doi:10.1016/j.semarthrit.2011.07.003
- Khatib Y, Madan A, Naylor JM, et al. Do Psychological Factors Predict Poor Outcome in Patients Undergoing TKA? A Systematic Review. Clin Orthop Relat Res. 2015; 473(8): 2630-2638. doi:10.1007/s11999-015-4234-9
- March MK, Harmer AR, Dennis S. Does Psychological Health Influence Hospital Length of Stay Following Total Knee Arthroplasty? A Systematic Review. Arch Phys Med Rehabil. 2018; 99(12): 2583-2594. doi:10.1016/j.apmr.2018.03.020
- Roth ML, Tripp DA, Harrison MH, et al. Demographic and psychosocial predictors of acute perioperative pain for total knee arthroplasty. Pain Res Manag. 2007; 12(3): 185-194. doi:10.1155/2007/394960
- Slim K, Nini E, Forestier D, et al. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003; 73(9): 712-716. doi:10.1046/j.1445-2197.2003.02748.x
- Ackley BJ, Ladwig GB, Swan BA, et al. Evidence-based nursing care guidelines-E-book: medical-surgical interventions. Elsevier Health Sciences. 2007.
- Cunningham DJ, DeOrio JK, Nunley JA, et al. The Effect of Patient Characteristics on 1 to 2-Year and Minimum 5-Year Outcomes After Total Ankle Arthroplasty. J Bone Joint Surg Am. 2019; 101(3): 199-208. doi:10.2106/JBJS.18.00313
- Cunningham DJ, Steele JR, Allen NB, et al. The Impact of Preoperative Mental Health and Depression on Outcomes After Total Ankle Arthroplasty. J Bone Joint Surg Am. 2021; 103(2): 131-138. doi:10.2106/JBJS.20.00395
- Conti MS, Caolo KC, Cororaton AD, et al. Preoperative PROMIS Physical Function Scores Predict Postoperative Outcomes Following Total Ankle Replacement. Foot Ankle Orthop. 2021; 6(3): 24730114211020336. doi:10.1177/24730114211020335
- Wilson JM, Schwartz AM, Farley KX, et al. Preoperative Depression Influences Outcomes Following Total Ankle Arthroplasty. Foot Ankle Spec. 2022; 15(4): 321-329. doi:10.1177/1938640020951657
- Kim TY, Lee HW, Jeong BO. Influence of Depressive Symptoms on the Clinical Outcomes of Total Ankle Arthroplasty. J Foot Ankle Surg. 2020; 59(1): 59-63. doi:10.1053/j.jfas.2019.07.001
- Steele JR, Cunningham DJ, Green CL, et al. Patient Characteristics of Possible Responders and Nonresponders to Total Ankle Arthroplasty. Foot Ankle Int. 2020; 41(8): 893-900. doi:10.1177/1071100720926123
- Mulligan RP, McCarthy KJ, Grear BJ, et al. Psychosocial Risk Factors for Postoperative Pain in Ankle and Hindfoot Reconstruction. Foot Ankle Int. 2016; 37(10): 1065-1070. doi:10.1177/1071100716655142
- Pugely AJ, Lu X, Amendola A, et al. Trends in the use of total ankle replacement and ankle arthrodesis in the United States Medicare population. Foot Ankle Int. 2014; 35(3): 207-215. doi:10.1177/1071100713511606
- Sedgwick P. Bias in observational study designs: cross sectional studies. BMJ. 2015; 350: h1286. doi:10.1136/bmj.h1286
- Brody DJ, Pratt LA, Hughes JP. Prevalence of Depression Among Adults Aged 20 and Over: United States, 2013-2016. NCHS Data Brief. 2018; (303): 1-8.
- Mental Health By the Numbers | NAMI: National Alliance on Mental Illness. Accessed September 27, 2022. https://www.nami.org/mhstats
- Pan X, Wang J, Lin Z, et al. Depression and Anxiety Are Risk Factors for Postoperative Pain-Related Symptoms and Complications in Patients Undergoing Primary Total Knee Arthroplasty in the United States. J Arthroplasty. 2019; 34(10): 2337-2346. doi:10.1016/j.arth.2019.05.035
- Chapman Z, Shuttleworth CMJ, Huber JW. High levels of anxiety and depression in diabetic patients with Charcot foot. J Foot Ankle Res. 2014; 7: 22. doi:10.1186/1757-1146-7-22
- Paget LDA, Tol JL, Kerkhoffs GMMJ, et al. Health-Related Quality of Life in Ankle Osteoarthritis: A Case-Control Study. Cartilage. 2021; 13(1_suppl): 1438S-1444S. doi:10.1177/19476035211025814
- Holt M, Swalwell CL, Silveira GH, et al. Pain catastrophising, body mass index and depressive symptoms are associated with pain severity in tertiary referral orthopaedic foot/ankle patients. J Foot Ankle Res. 2022; 15(1): 32. doi:10.1186/s13047-022-00536-5
- Poleshuck EL, Bair MJ, Kroenke K, et al. Psychosocial stress and anxiety in musculoskeletal pain patients with and without depression. Gen Hosp Psychiatry. 2009; 31(2): 116-122. doi:10.1016/j.genhosppsych.2008.10.003
- DiLiberto FE, Aslan DH, Houck JR, et al. Overall Health and the Influence of Physical Therapy on Physical Function Following Total Ankle Arthroplasty. Foot Ankle Int. 2020; 41(11): 1383-1390. doi:10.1177/1071100720942473
- Ahn DH, Lee YJ, Jeong JH, et al. The effect of post-stroke depression on rehabilitation outcome and the impact of caregiver type as a factor of post-stroke depression. Ann Rehabil Med. 2015; 39(1): 74-80. doi:10.5535/arm.2015.39.1.74
- Paolucci S, Antonucci G, Pratesi L, et al. Poststroke depression and its role in rehabilitation of inpatients. Arch Phys Med Rehabil. 1999; 80(9): 985-990. doi:10.1016/s0003-9993(99)90048-5
- Cabello M, Miret M, Caballero FF, et al. The role of unhealthy lifestyles in the incidence and persistence of depression: a longitudinal general population study in four emerging countries. Global Health. 2017; 13(1): 18. doi:10.1186/s12992-017-0237-5
- Mahomed NN, Liang MH, Cook EF, et al. The importance of patient expectations in predicting functional outcomes after total joint arthroplasty. J Rheumatol. 2002; 29(6): 1273-1279.
- Halawi MJ, Chiu D, Gronbeck C, et al. Psychological Distress Independently Predicts Prolonged Hospitalization After Primary Total Hip and Knee Arthroplasty. J Arthroplasty. 2019; 34(8): 1598-1601. doi:10.1016/j.arth.2019.03.063
- Bressi SK, Marcus SC, Solomon PL. The impact of psychiatric comorbidity on general hospital length of stay. Psychiatr Q. 2006; 77(3): 203-209. doi:10.1007/s11126-006-9007-x
- Elenkov IJ. Systemic stress-induced Th2 shift and its clinical implications. Int Rev Neurobiol. 2002; 52: 163-186. doi:10.1016/s0074-7742(02)52009-2
- Ghoneim MM, O’Hara MW. Depression and postoperative complications: an overview. BMC Surg. 2016; 16: 5. doi:10.1186/s12893-016-0120-y