
Comparison of Methamphetamine Induced Psychosis and Primary Psychotic Disorder: Scoping Review of Social Cognition
Felix Diotte1, Stephane Potvin2, Donna Lang3, Amal Abdel-Baki4, Alicia Spidel5, Marie Villeneuve6, Tania Lecomte1*
1Departement of psychology, University of Montréal
2Departement of psychiatry and addiction, University of Montréal, Canada,
3Department of Radiology, University of British Columbia, Canada,
4Centre hospitalier de l'Université de Montréal, Canada,
5University of Fraser Valley, Fraser Health, Canada,
6Institut universitaire en santé mentale de Montréal, Canada
Abstract
As many as 43% of methamphetamine users will have a psychotic episode in their lifetime. Of these, 30% will develop a primary psychotic disorder, such as schizophrenia. The current state of the literature does not currently allow us to determine who will develop a primary psychotic disorder following a methamphetamine-induced psychosis (MIPD). This distinction is important, since people with a first episode of a psychotic disorder need specific and rapid treatments to ensure optimal recovery. Social cognition could help predict distinct profiles. The aim of this scoping review is to evaluate the literature in order to extract the differences between MIPD and primary psychotic disorders in the domain of social cognition. Articles were recovered from PsychINFO, Medline and Web of science and were retained if they met the following inclusion criteria: (a) original research or meta-analyses, (b) complete or partial sample with a psychotic disorder diagnosis with comorbid methamphetamine use, or MIPD, (c) studies focusing on the difference between a methamphetamine-induced psychosis and a primary psychotic disorder, and (d) studies focusing on social cognition in psychotic or methamphetamine using population. A total of 17 articles were identified, with none directly aiming at distinguishing MIPD and primary psychotic disorder using social cognition. Future studies on social cognition are needed in order to determine differences in the severity of deficits between the two profiles.
Introduction
According the World drug report1, 34 million people across the globe used methamphetamine (METH) in 2015. Although recent years have seen a surge in opioids, such as Fentanyl, METH is seeing a new come back with a reported increase of 487 % in urine drug test (over 1 million tested) from 2013 to 20192. METH’s popularity is due to it being highly addictive3 and not expensive4. The rewarding effects of the drug leads to high addiction rates and rapid escalation of use in those developing a disorder. According to users, METH triggers sensations of increased energy, euphoria, feelings of sexual excitement, control, and mastery of their surroundings as well as a sense of overall well-being. METH can however also induce fever, cardiac arrhythmia, nausea, increased heart rate and blood pressure, agitation, confusion, aggressive behaviour anxiety, panic attacks and psychotic symptoms, namely auditory hallucinations and paranoid delusions5.
Chronic METH abuse can cause cognitive and social impairments, suicidal thoughts and behaviors, and long-term structural brains changes5-7. As such, several cognitive deficits are documented in chronic METH users, such as decreased performance in attention, speed of processing, verbal and working memory, response inhibition, problem-solving and decision-making when compared to non-using healthy controls5,8,9. In most of the latter cognitive domains, the amplitude of the cognitive deficits observed are moderate, whereas visual learning and visuospatial skills deficits have also been observed but are generally of lower amplitudes.
According to Sommers and colleagues3, most METH users experience severe psychiatric symptoms like depression, psychosis, with as many as 38% reporting experiencing auditory or visual hallucinations. According to a recent meta-analysis, a median of 43% of METH users will experience a METH-induced-psychotic-disorder (MIPD) in their lifetime10. Of those, close to 30% will see their diagnosis change to that of a first psychotic episode of a schizophrenia-spectrum disorder11. Schizophrenia, like most primary psychotic disorders, is a severe mental disorder necessitating specific services and treatments, with better prognosis and recovery when these are offered early and in a ‘youth-friendly’ manner, i.e. adapted to youth’s needs12. Unfortunately, there is no reliable method to detect which individuals will go on to develop a first episode of a primary psychotic disorder after a MIPD13. METH, like other drugs (e.g. cannabis), can act as a trigger, precipitating a first psychotic episode in individuals vulnerable to developing psychotic illnesses such as schizophrenia. Individuals receiving emergency psychiatric care following a MIPD receive an uncertain diagnosis, given 3 to 6 months of persistent symptoms are necessary to confirm a diagnosis of a primary psychotic disorder14. Without a proper diagnosis, individuals can find themselves in-between services and without appropriate treatment, with important consequences on their rehabilitation and recovery. Misdiagnosis, or absence of a clear diagnosis, can result in patients not receiving the appropriate and needed treatment. For instance, individuals seeking help for MIPD are often sent home after a brief hospitalization, with some psychoeducation about the negative effects of methamphetamine use, whereas individuals at risk of schizophrenia need to receive intensive services from an early psychosis intervention service15. Should early psychosis intervention services not be offered quickly, a longer period of untreated psychosis would follow, which has been linked to worse recovery outcomes and increased risks of psychotic relapse16. Relapses imply rehospitalizations, which increase the risk, for those concerned, of losing their job, their housing situation and also increases the likelihood of developing symptoms that are treatment resistant17,18.
Despite being hard to estimate, inadequate treatment of individuals with psychotic disorders is also costly13,19. Direct costs include repeated hospitalisations, whereas indirect costs include unemployment, social isolation, and financial impact on families. Cheung and colleagues found that the cost of treating patients admitted to the hospital, mainly due to psychotic relapses, was about 18.5 times higher than the cost of treating outpatients20. This indicates that preventing hospitalization of individuals with psychotic symptoms is both economically and socially desirable. The prevention of hospitalization would be best supported by determining as soon as possible, after the first contact with mental health services (such as emergency rooms consultations, psychiatric hospitalisations, psychiatric outpatient evaluations), who is at risk of developing a primary psychotic disorder. By determining who is at greater risk of developing a primary psychotic disorder as soon as possible, we could ensure that these individuals get appropriate treatments sooner and, therefore, prevent worsening of psychotic symptoms, cognitive deficits and numerous other dire consequences.
To date, several studies have attempted to distinguish those with MIPD who are clearly in a psychotic state linked with METH use and will recover without further symptoms from those who will eventually receive a schizophrenia-spectrum disorder diagnosis. These studies have looked at specific psychotic symptoms (content, type and severity) in those with MIPD21-23 and in those with a primary psychotic disorder24-26. It has been suggested that auditory hallucinations are present in both diagnoses whereas visual hallucinations seem more prominent in MIPD11,27,28, as in many substance-induced psychoses. However, these studies often conclude that an important overlap in the symptoms reported makes it hard to reach a strong conclusion. In fact, Bramness and colleagues29 concluded that the clinical symptoms in both conditions were too similar to distinguish them based solely on that information. Wearne and Cornish’s review concluded that general positive symptoms (i.e. delusions and hallucinations) are similar in MIPD and schizophrenia, both in terms of prevalence and severity11. The main difference found in their review was the suggestion that negative symptoms might differ between both groups. The frequency and severity of some negative symptoms (i.e. flattened affect and social withdrawal) appeared reduced in MIPD compared with negative symptoms documented in a primary psychotic disorder. It is important to mention that METH users also frequently present with depressive symptoms5, which can mimic negative symptoms, making the distinction between both difficult.
Other researchers have examined neurocognition as a potential marker to distinguishing MIPD from more persistent psychotic disorders, showing major deficits in people with METH use, in people with schizophrenia and in the MIPD population11,30,31. As mentioned, specific cognitive deficits are often observed in METH users. Similarly, cognitive deficits across several neurocognitive domains have also been documented in different meta-analyses and reviews in individuals presenting with a first episode of a primary psychotic disorder, including deficits in attention, processing speed, executive functioning, episodic and working memory, and fine motor skills30,32,33. According to a recent review11, the cognitive impairments in both disorders can initially appear similar, although a closer look can suggest different effect sizes in terms of severity of the measured deficits (with people using METH faring better than those with schizophrenia). Selective visual attention11 and visual memory34 deficits seem less pronounced in MIPD than in schizophrenia, in the few studies having compared them.
Currently, psychotic symptoms and neurocognitive deficits have not allowed clinicians to discriminate between those with a clear MIPD and those with a first episode of a primary psychotic disorder. Social cognition has infrequently been studied as a potential domain of interest, despite the fact that it appears impaired in individuals with schizophrenia (see Kalkstein’s review30) and also in METH users35,36. Three recent meta-analyses on cognition in METH users looked at neurocognition but did not to investigate social cognition36-38. Social cognition refers to cognitive skills used to interact with, and understand, other individuals’ emotions, intentions and actions39. Unsurprisingly, social cognition was analysed in only 3 of the 44 studies in Potvin’s meta-analysis35, showing strong preliminary results for social cognition deficits in individual with METH use, but highlighting the need to do more research on the subject. Using social cognition as a differentiating factor might help determinate who needs specific treatments for persistent psychosis.
Although it is well known that social cognition is impaired in schizophrenia30,40, and in METH users35,36,41, very few studies seem to have looked at these deficits in MIPD population. It therefore appears worthy to clarify the current state of the literature on social cognition in people with concurrent METH use and psychosis, to determine if more studies should consider social cognition when attempting to distinguish those with MIPD from those with a primary psychotic disorder triggered by METH. Distinguishing the two diagnoses would help clinicians to orientate patients towards more appropriate treatments and inevitably help with their rehabilitation.
Methods
The extent of the literature being too narrow for a meta-analysis, we propose a scoping review in order to evaluate the literature of the last 20 years regarding potential differences between MIPD and primary psychotic disorders in the domain of social cognition. Scoping reviews present a broad overview of the evidence pertaining to a topic, and are useful when examining emerging research domains in order to clarify key concepts and identify gaps42. As such, we followed the scoping review methodology proposed by Arksey and O’Malley43.
The following research question was used to help guide our article search: Are social cognitive deficits different in individuals with MIPD from those found in individuals with a primary psychotic disorder (schizophrenia spectrum) triggered by METH use?
Considering that few studies directly compared METH-psychosis and primary psychotic disorders (schizophrenia spectrum) on social cognition, we chose to also document results of studies looking specifically at social cognition in samples of people with:
1. METH-psychosis;
a) Should few studies with METH-psychosis samples emerge, we would expand to studies with individuals with METH use who DID NOT exclude those with a history of psychotic symptoms.
2. primary psychotic disorders (schizophrenia spectrum) and METH use (or stimulants);
b) Should few studies with comorbid psychotic disorder and METH use (or stimulants) emerge, we would expand to studies with individuals with schizophrenia or other primary psychotic disorder who DID NOT exclude those with stimulant or substance misuse.
Search strategy
The following terms and keywords were used to retrieve articles form PsychINFO, MEDline and Web of science: (psychosis or psychoses or “psychotic disorder” or schizophren* or “severe mental disorder”) AND (methamphetamine or speed or stimulants or “substance induced” or “psychostimulant” or meth) AND (social perception or emotion recognition or theory of mind or attributional bias or emotion regulation). Only the articles published between January 2000 and September 2020 have been retained.
Inclusion and exclusion criteria
Peer-reviewed articles that were available in English or in French were included. Studies that met the following criteria were included: (a) original research or meta-analyses, (b) complete or partial sample with a psychotic disorder diagnosis (i.e., schizophrenia, first-episode psychosis, schizoaffective disorder, schizophreniform disorder) or a substance-induced psychosis, (c) studies focusing on the difference between a substance induced psychosis and a psychotic disorder, and (d) studies focusing on social cognition in psychotic or methamphetamine using population. The exclusion criteria, were the following: (a) sample composed of children and adolescents; (b) animal research, pharmacotherapy research or genetic research, (c) qualitative data only and (d) study excluded people with psychotic symptoms (in METH users) or with a comorbid substance abuse (in schizophrenia). This latter criterion was important since many studies have investigated social cognition in schizophrenia for instance but have systematically excluded those who used or abused substances (including stimulants). Similarly, many studies on methamphetamine misuse have excluded participants who mentioned having experienced psychotic symptoms. Given the research question, it was important that people with comorbid presentations of psychotic symptoms and substance misuse be included in the studies.
Data extraction
The articles were first screened by title, then by abstract by the first author. The abstracts were also screened by T. L. Discussions took place to resolve any disagreements regarding the chosen articles. The final selection of full-text articles was completed after a consultation with T. L.
Quality assessment
Although scoping reviews do not usually entail quality assessments, we nonetheless verified the quality of the studies (authors F. D. and T. L). Both authors independently assessed the quality of each study using the National Institute of Health (NIH) Quality Assessment Toolsa, and then a consensus discussion took place, where the rating of each study were compared. According to the methodology used, the quality assessment generated binary scores (yes/no) for the power of the study (sample size), objective clearly established, selection of participants, the inclusion and exclusion criteria, use of validated assessments, and control for confounding variables. The agreement rate was perfect for 80% of the studies, with a single-point discordance (on a maximum score of 12 or 14 points) for 20% of the ratings. These studies were further discussed until an agreement was reached.
a https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Analysis
The classification of studies was based on the population in the studies (i.e., individuals with schizophrenia, individuals with a first episode psychosis, individuals with a METH use disorder, individuals with a METH use disorder and individuals with a history of psychosis or at ultra-high risk of developing a psychotic disorder). We also documented the country where the research was conducted. The classification was chosen after a consensus among the authors.
Results
The search strategy produced a total of 258 abstracts. The inclusion and exclusion criteria were then applied, leaving 73 articles, 58 of which were taken out after full text verifications. Of those 58 articles, 50% (29 articles) were excluded because the studies excluded individuals with psychotic symptoms (in the case of METH studies) or excluded those with a psychotic disorder and comorbid substance use disorder or even any substance use (for psychotic disorder or schizophrenia studies). See Figure 1- PRISMA Flow diagram.
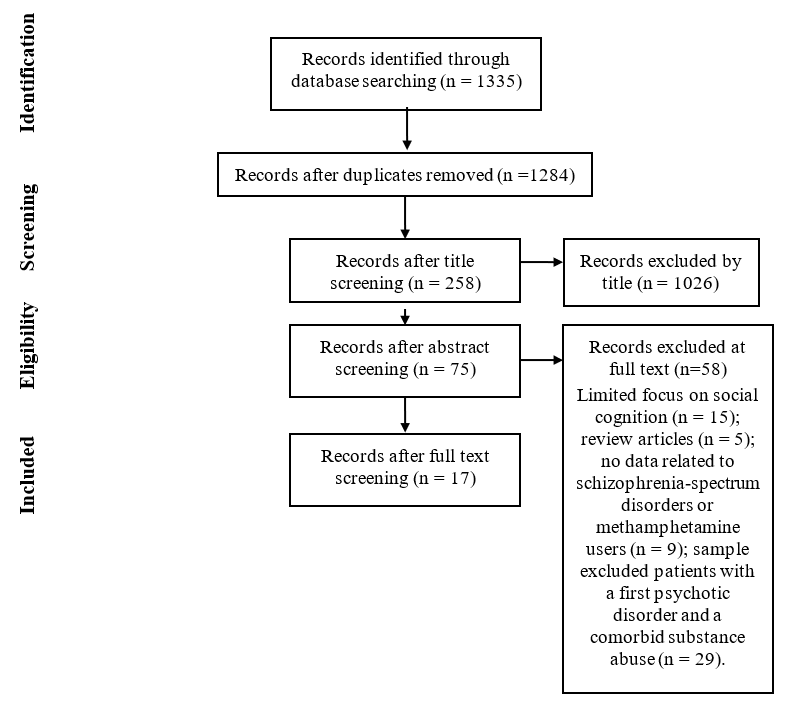
Figure 1: PRISMA flow diagram
Characteristics of Selected Studies
Only 17 articles were eligible (see Table 1). Studies were from the Netherlands (n = 5), the United States (n = 2), Norway (n = 2) Australia (n = 2), Belgium (n = 1), England (n = 1), South Africa (n = 1) and Spain (n = 1). Sample sizes ranged from 26 to 2,217 (for a meta-analysis) There was a total of 2,795 participants with a psychotic disorder, 91 participants with a nonpsychotic diagnosis and 1,993 participants with no psychiatric diagnosis. Most studies (n = 10) used a structured or semi structured interview to assess or confirm the diagnosis. More than 60 different tests and questionnaires were used across all 17 studies to assess different dimensions of cognition, including 10 different tests for social cognition. As was found for neurocognition, the assessment of social cognition was not standardized. Most of the studies included only a small clinical sample and were conducted in a single site (convenience sample). None of the studies had conducted a power analysis, and most mentioned underpower as a limitation. Most used a cross-sectional study design and more than half of the studies (65%) used a healthy control group. The quality score attributed to the articles ranged from 55% to 100%, with a mean of 68%, suggesting a moderate quality level (see Table 1).
Table 1: Summary of Selected Studies
|
|
Authors
|
Country |
Diagnoses Of Population(S) Studied |
Sample Size, Age, Sex |
Study Design |
Instruments Used |
Key Findings |
Quality Assessment* |
|
Social cognition in patients with schizophrenia related articles (n = 6) |
Barkhof, E., de Sonneville, L. M., Meijer, C. J., & de Haan, L. (2015) |
Netherlands |
Schizophrenia and schizoaffective disorder (n = 42); healthy controls (n = 42) |
N=84
Clinical sample: Age M= 38.4 ± 9.7 Sex= 71% M
Controls: Age M= 41.2 ± 11.8 Sex= 71% M |
Cross-sectional with controls |
-ANT - SCID-I for DSM-IV - Face Recognition - Identification of Facial Emotions - Baseline speed |
- Clinical patients were slower and less accurate in recognising facial emotions than healthy controls.
- Clinical patients showed more difficulties processing social information than non-social information (F(3,237) = 2.407, p = .068, η = 0.030). - Clinical patients were less accurate at identifying negative emotions than controls, but not in positive emotions (F(4,316) = 4.949, p = .001, η = 0.058). |
73% |
|
Pijnenborg, G. H. M., Spikman, J. M., Jeronimus, B. F., & Aleman, A. (2013) |
Netherlands |
Schizophrenia (n = 46); healthy controls (n = 53) |
N = 99
Clinical sample: Age M=27.4 ± 7.7 Sex= 74% M Controls: Age M= 31.1 ± 10.2) Sex= 46% M
|
Cross-sectional with controls |
-CIDI - PANSS - Emotional prosody task - FEEST - Faux Pas test, short version - EEQ - GIT - 15-Words Test - Six Elements Test of the Behavioural Assessment of the Dysexecutive Syndrome - TMT |
- Affective empathy and affective ToM put together explains almost half (45%) of the variance in insight (F(2,43) = 17,38, p < .01).
|
64% |
|
|
Schenkel, L. S., Spaulding, W. D., & Silverstein, S. M. (2005) |
United States |
Schizophrenia (n = 23); Schizoaffective Disorder (n = 19) |
N = 42
Age M=41.7 ± 10.5 Sex= 60% M |
Cross-sectional |
-BPRS - Hinting Task - Hayling Sentence Completion Test - Brixton Spatial Anticipation Test - COWAT - Contour Integration Test - Shipley Institute of Living Scale |
- A better performance on the Hinting Task was associated with a better performance in generating more appropriate verbal responses (r = 0.47, p < .005). - Poor ToM performance was associated with deficits in visual, perceptual and linguistic context processing.
|
55% |
|
|
Mangelinckx, C., Belge, J. B., Maurage, P., & Constant, E. (2017). |
Belgium |
Schizophrenia (n = 32); healthy controls (n = 32) |
N = 32 Clinical sample: Age M=47.3 ± 10 Sex= 53% M
Controls: Age M=46.4 ± 10.5 Sex= Not provided |
Cross-sectional with controls |
- PANSS - State and Trait Anxiety Inventory A-B - Beck Depression Inventory, short version - Simple Reaction Time - Radboud Face Battery |
- Patients were slower (F(1, 60) = 17.628, p < .001) and less accurate (F(1, 60) = 28.969, p < .001) than controls on emotional conditions whatever the stimulus type was. |
64% |
|
|
Sjølie, C., Meyn, E. K., Raudeberg, R., Andreassen, O. A., & Vaskinn, A. (2020). |
Norway |
Schizophrenia (n = 69); schizoaffective disorder (n = 22) |
N = 91
Age M=29.1 ± 8.4 Sex= 63% M
|
Cross-sectional
|
- SCID for DSM-IV axis 1 -PANSS -GAF -WASI -MASC -MCCB -BVMT-R |
- Non-social cognition is responsible for 17% of the variance in ToM. - ToM performance was not predicted by any of the non-social cognitive tests. |
55% |
|
|
Vaskinn, A., Sundet, K., Friis, S., Simonsen, C., Birkenaes, A. B., Jonsdottir, H., Ringen, P. A. & Andreassen, O. A. (2008) |
Norway |
Schizophrenia (n = 26) |
N = 26
Age M=32.3 ± 9.3 Sex= 65% M
|
Cross-sectional |
- SCID for DSM-IV axis 1 - PANSS - WASI - NART - GAF - SFS - MATRICS - Face/Voice Emotion Identification and Discrimination Test - WCST - AIPSS |
-Emotion perception acts as a mediator in the relationship between social problem-solving and neurocognition because it’s in relation with both the independent variable (r = .67, p <.001) and the dependant variable (r = .50, p < .001).
|
64% |
|
|
Social cognition in patients with first episode psychosis related articles (n = 5) |
Simons, C. J., Bartels-Velthuis, A. A., Pijnenborg, G. H., & Genetic Risk and Outcome of Psychosis (GROUP) Investigators. (2016) |
Netherlands |
Non-affective psychotic disorder (n = 745); Healthy controls (n = 447) |
N = 1192 Clinical sample: Age M=30.2 ± 7.2 Sex= 76% M
Controls: Age M=34.1 Sex= 44% M
|
Cohort study |
- CASH interview -SCAN -PANSS -WAIS-III Short form -CPT -WLT -RST -DFAR -Hinting Task -SFS |
- Social cognition is not predictive of social functioning (p > .10). |
82% |
|
Ayesa-Arriola, R., Setién-Suero, E., Neergaard, K. D., Ferro, A., Fatjó-Vilas, M., Ríos-Lago, M., Otero, S., Rodriguez-Sancehz, J. M. & Crespo-Facorro, B. (2016) |
Spain |
Schizophrenia (n = 87); schizophreniform disorder (n = 40); brief psychotic disorder (n = 22) psychosis non specified (n = 11); Healthy controls (n = 159) |
N = 319 Clinical sample: Age M=32.2 ± 10.8 Sex= 54% M
Controls: Age M=29.1 ± 7.9 Sex= 61% M
|
Cross-sectional with controls |
-SCID-I -CASH -SANS -SAPS -CDSS -RAVLT -RCF -WAIS-III -TMT -Grooved Pegboard Test -CPT -Reading the Mind in the Eyes
|
-Clinical sample had significantly lower ToM scores than controls at baseline, 1-year and 3-years follow-up (F = 31; p < .001). -There were significant differences in all neurocognitive domains at baselines between the ToM deficit and non-deficit groups (p < .017). -The same differences were seen at 1-year follow ups (except in visual memory and executive functions) and 3-year follow ups (working memory and executive functions). - Lower ToM scores were associated with greater neurocognitive deficits (especially processing speed (p < .001)).
|
64% |
|
|
Danaher, H., Allott, K., Killackey, E., Hester, R., & Cotton, S. (2018) |
Australia |
First episode psychosis disorder (n = 134); Healthy controls (n = 46) |
N = 180 Clinical sample: Age M=20.2 ± 2.4 Sex= 67% M
Controls: Age M=20.5 ± 2.6 Sex= 61% M |
Cross-sectional with controls |
-Socio-demographic questionnaire - WRAT-4 - SCID-I - BPRS - SANS - SOFAS - WAIS-III - RCFT - RAVLT - SDMT - TMT -COWAT - Animal Fluency Test - DANVA - False Belief and Deception Stories Task - PST - Hinting task |
-No sex differences in social cognition (p = .277). |
64% |
|
|
Stouten, L. H., Veling, W., Laan, W., van der Helm, M., & van der Gaag, M. (2017) |
Netherlands |
Schizophrenia (n = 81), Schizo-affective disorder (n = 9), Brief psychotic disorder (n = 9), Delusional disorder (n = 5), Shared psychotic disorder (n = 2), Non-specified psychotic disorder (n = 56) |
N = 162 Clinical sample: Age M=27.6 ± 6.3 Sex= 71 % M
|
Cross-sectional
|
-SCAN - IRAOS -PANSS -BDI -BAI -PSP -ANT -Hinting task -WAIS-III -DACOBS -CPT -TMT -RAVLT -BVMT |
-There is a strong association between general social cognition and impaired psychosocial functioning. -Together, social cognitive biases, emotion processing speed, general social cognition and attribution and inference bias can explain 71.93% of the variance in psychosocial functioning. |
64% |
|
|
Van Hooren, S., Versmissen, D., Janssen, I., Myin-Germeys, I., à Campo, J., Mengelers, R., van OS, J. & Krabbendam, L. (2008) |
Netherlands |
Schizophrenia (n = 31), schizoaffective disorder (n= 3), Non-specified psychotic disorder (n = 10), Healthy controls (n = 54), Non-psychotic first degree relatives (n = 47), High level of psychotic experiences (n = 41) |
N = 186 Age: Not provided for any sample Sex: Not provided for any sample |
Cross-sectional
|
-SCWT -TMT -Semantic Fluency -Hinting task -Beads task -ART -SAT -IPSAQ |
-In psychosis, neurocognition and social cognition represent two separate areas of vulnerability. -Social cognition might be a multidimensional construct. -All neurocognitive measures are correlated with the Hinting task. |
64% |
|
|
Social cognition in patients with METH use with a history of psychosis related articles (n = 2) |
Arunogiri, S., Verdejo-Garcia, A., McKetin, R., Rubenis, A. J., Fitzpatrick, R. E., & Lubman, D. I. (2019) |
Australia |
METH using participants with psychosis (n = 29) METH using participants without psychosis (n = 70), Healthy controls (n = 32) |
N = 131 Clinical sample: Age M=32.2 ± 1.2 Sex= 75% M
Controls: Age M=32.4 ± 1.7 Sex= 69% M |
Cross-sectional with controls |
-SCID -BPRS -Timeline Followback -SDS -IGT -DDT -EFT
|
-METH-using individuals with psychosis showed poorer scores at emotion recognition than METH-using individuals without psychosis (p < .001). -Recognition of anger and sadness were specifically impaired in METH-using individuals with psychosis. |
64% |
|
Uhlmann, A., Ipser, J. C., Wilson, D., & Stein, D. J. (2018) |
South Africa |
METH using participants with psychosis (n = 20) METH using participants without psychosis (n = 21), Healthy controls (n = 21) |
N = 62 Clinical sample: Age M=23.5 ± Not provided Sex= 80% M
Controls: Age M=24 ± Not provided Sex= 80% M |
Cross-sectional with controls |
-SCID -PANSS -ERT -RMET -AQ -BDI-II |
-Both METH using participants with psychosis (p < .001) and METH using participants without psychosis (p = .047) received lower social cognition scores than controls. -METH using participants with psychosis scores were lower than METH using participants without psychosis (p = .040). - METH using participants with psychosis showed deficits in recognising all 4 basic emotions (anger, fear, happiness and sadness), whereas METH using participants without psychosis’ deficit were restricted to anger. |
73% |
|
|
Social cognition in ultra-high risk individual related articles (n = 2) |
Corcoran, C. M., Keilp, J. G., Kayser, J., Klim, C., Butler, P. D., Bruder, G. E., Gur, C. R. & Javitt, D. C. (2015) |
United States |
Ultra high risk of first psychotic disorder (n = 49), Healthy controls (n = 31) |
N = 80 Clinical sample: Age M=20.4 ± 4.4 Sex= 66% M
Controls: Age M=21.4 ± 3.1 Sex= 65% M |
Cross-sectional with controls |
-SIPS/SOPS -ER40 -WAIS-III -EMODIFF -AER -MATRICS -MCCB -CPT-IP |
-Ultra high-risk patients who developed a first psychotic disorder showed more deficits in emotion recognition task than Ultra high-risk patients who didn’t develop a first psychotic disorder (p = .006). -Deficits in emotion recognition exist in ultra high-risk patients before the onset of schizophrenia. |
64% |
|
Fusar-Poli, P., Deste, G., Smieskova, R., Barlati, S., Yung, A. R., Howes, O., Stieglitz, R.-D., Vita, A., McGuire, P. & Borgwardt, S. (2012) |
England |
Ultra high risk of first psychotic disorder (n = 1 188), Healthy controls (n = 1 029) |
N = 2 217 Clinical sample: Age M=20 ± 3.4 Sex= 66% M
|
Meta-analysis |
-TMT-B -LNS -Digit span task -RAVLT -CVLT -WMS -VRI -CPT -Reaction time tasks -TMT-A -DSST -Finger tapping test -VF semantic fluency task -VF phonological fluency task -Block design test -WCST
|
-Despite being able to recognize that social cognition is impaired when compared to healthy controls, there was not enough data to analyse the transition to psychosis. |
100% |
|
|
Social cognition in METH users related article (n = 2) |
Hanegraaf, L., Arunogiri, S., Hohwy, J., & Verdejo-Garcia, A. (2020) |
Australia |
METH dependence (n = 86) |
N = 86 Clinical sample: Age M=30.7 ± 6.7 Sex= 80% M
|
Cross-sectional |
-SCID -WASI-II -PBQ-SF -EFT |
-High levels of dysfunctional beliefs are associated with poor fear recognition. -Neither paranoid nor antisocial personality beliefs were a significant predictor of fear recognition. -A positive association was found between the misclassification of emotions as disgust and passive-aggressive personality belief (r = 0.34, p = .002). |
73% |
|
Kim, Y. T., Kwon, D. H., & Chang, Y. (2011) |
Korea |
METH abuse (n = 28),
Healthy controls (n = 27)
|
N = 55 Clinical sample: Age M=40.2 ± 7. Sex= 100% M
Controls: Age M=39.9 ± 3.3 Sex= 100% M |
Cross-sectional with controls |
- Facial Emotion Recognition Task - RMET -Hinting task -WCST |
- METH abusers obtained lower score than healthy subjects in the Facial Emotion Recognition Task (t = 3.03, df=34.67, p = 0.004) and specially in with fearful expression (t = 3.22, df=39.54, p = 0.003). - METH abusers also obtained lower score then healthy subjects in the RMET (t = 3.75, df=53, p <0.001) and Hinting Task (t = 2.09, df=37.371, p = 0.04). -There is a correlation between the total score of the Facial Emotion Recognition Task with the RMET (r = 0.423, p = 0.025). |
73% |
*Quality assessment done with the Study Quality Assessment Tools of the National Institutes of Health (NIH) ( https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools)
Note: AER, Auditory emotion recognition AIPSS Assessment of Interpersonal Problem-Solving Skills, ANT, Amsterdam Neuropsychological Tasks; AQ, Buss and Perry Aggression Questionnaire; ART, Action Recognition Test; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BPRS, Brief Psychiatric Rating Scale; BVMT-R, Brief Visuospatial Memory Test—Revised; CASH, Comprehensive Assessment of Symptoms and History; CDSS, Calgary Depression Scale for Schizophrenia; CIDI, Composite International Diagnostic Interview; COWAT, Controlled Oral Word Association Test; CPT, Continuous Performance Test-HQ; CPT-IP, Continuous Performance Test-Identical Pairs; CVLT, California Verbal Learning Test; DACOBS, Davos Assessment for Cognitive Biases Scale; DANVA, Diagnostic Analysis of Nonverbal Accuracy-2—Adult Version; DDT, Delay Discounting Task DFAR, Degraded Facial Affect Recognition; DSST, Digit Symbol Substitution Test; EEQ, Emotional Empathic tendency scale; EFT, Ekman Faces Test; EMODIFF, Penn Emotion Discrimination Task; ER40, Penn Emotion Recognition Test – 40 faces; ERT, Emotion Recognition Task; FEEST, Facial Expression of Emotion: Stimuli and Tests; GAF, Global Assessment of Functioning; GIT, Groninger Intelligence Test; IGT, Iowa Gambling Task; IPSAQ, Internal, Personal and Situational Attributions Questionnaire; IRAOS, Retrospective Assessment of the Onset of Schizophrenia; LNS, Letter Number Sequencing task; MASC, Movie for the Assessment of Social Cognition; MATRICS, Measurement and Treatment Research to Improve Cognition in Schizophrenia; MCCB, MATRICS Consensus Cognitive Battery; METH: Methamphetamine NART, National Adult Reading Test, PANSS, Positive and Negative Syndrome Scale; PBQ-SF, Personality Belief Questionnaire- Short Form; PSP, Personal and Social Performance; PST, Picture Sequencing Task, RAVLT, Rey Auditory Verbal Learning Test; RCF, Ray Complex Figure; RCFT, Rey-Osterrieth Complex Figure Test; RMET, Reading Mind in the Eyes Task; RST, Response Shifting Task; SANS, Scale for the Assessment of Negative Symptoms; SAPS, Scale for the Assessment of Positive Symptoms; SAT, Speech Attribution Task, SCAN, Schedules for Clinical Assessment for Neuropsychiatry; SCID, Structured Clinical Interview; SCWT, Stroop Colour Word Test; SDMT, Symbol Digit Modalities Test; SDS, Severity of Dependence Scale, SFS, Social functioning Scale; SIPS/SOPS, Structured Interview for Prodromal Syndromes/Scale of Prodromal Symptoms; SOFAS, Social and Occupational Functioning Assessment Scale; TMT, Trail Making Test; ToM, Theory of Mind; VF, Verbal Fluency; VRI, Visual Reproduction Index; WASI, Wechsler Abbreviated Scale of Intelligence; WCST, Wisconsin Card Sorting Test; WLT, Word Learning Task; WMS, Wechsler Memory Scale; WRAT-4, Wide Range Achievement Test – Fourth Edition
Theme of Selected Studies
The 17 articles addressing social cognition were grouped according to their population sample in five different categories: (i) studies involving individuals with METH use and a history of psychosis (n = 2), (ii) studies involving individuals with schizophrenia (n = 6) that did not exclude stimulant use, (iii) studies individuals with a first episode psychosis (n = 5) that did not exclude stimulant use, (iv) studies involving individuals considered at ultra-high-risk of developing a psychotic disorder (n = 2) that did not exclude stimulant use, and (v) studies involving individuals with METH use alone (n = 2) that did not exclude psychotic disorders. Despite finding 2 articles including people with METH use and a history of psychosis, none tried to differentiate patients with a psychotic disorder from those who had a MIPD.
Individuals with METH Use and psychosis
To our knowledge, no study directly compared people with a primary psychotic disorder to METH users with psychosis on social cognition. Only two articles directly compared METH users with and without psychotic symptoms. The first article44 found that METH users with psychotic symptoms generally showed poorer scores on emotion recognition when compared to non-psychotic METH users (p < .001). A significant difference was also found between METH users with psychosis and healthy controls at correctly identifying discrete emotions; whereas no significant difference was found between non-psychotic METH users and healthy controls. These impairments were prominent when the emotion was anger or sadness. This result indicates a difference in the accuracy of emotion recognition between METH users with and without psychotic symptoms. The other study compared METH users with and without psychosis on their level of aggression, whilst considering emotion recognition45. There were no significant differences between the groups on aggression levels but both groups showed impaired emotion recognition skills. The impairments were greater in the group of METH users with psychosis. Whereas the METH users with psychosis showed impairment in recognising all 4 basic emotions (anger, fear, happiness and sadness), the METH users without psychosis only showed impairment related to anger.
Individuals with schizophrenia (stimulant use not excluded)
Of the 6 studies in this category, half of them looked at theory of mind (ToM) whereas the other half looked at emotion perception or recognition. Impairments in both of those concepts in individuals with schizophrenia (excluding those who use substances) has been clearly established. When compared with healthy controls, individuals with schizophrenia’s performance in different social cognition tasks were significantly worse46-48. ToM was compared to neurocognition in two studies of this review, attempting to determine if the concepts were intertwined or not49-51. Sjølie’s study51 found that neurocognition, such as visual and verbal memory, speed of processing and executive functions, was not predictive of ToM. Put together, the neurocognitive concepts measured explained 17% of the variance in ToM, though none uniquely predicted ToM performance. However, in Schenkel’s study49, poorer ToM capacity was associated with more disorganized symptoms and deficits in neurocognition, such as visual context processing. In Pijnenborg and colleagues’ study48, ToM was related to insight. Affective ToM, meaning the knowledge about emotions of other people, and affective empathy when put together explained 45% of the variance in insight. Different angles of research were also looked at regarding emotion perception or recognition in individuals with schizophrenia. In Mangelinckx and colleagues’ study47, the emotional stimulus was presented visually, vocally and both visually and vocally. When compared to controls, individuals with schizophrenia were slower and less accurate at emotion recognition, whatever the stimulus type was. Emotion perception was identified as a partial mediator in the relationship between neurocognition and social problem-solving51. A difference was found when identifying negative and positive emotions in individuals with schizophrenia, with lower scores than controls in the accuracy of identifying negative emotions but not in identifying positive emotions46. This finding indicates that recognising negative emotions might represent a specific difficulty for individuals with schizophrenia.
Individuals with first episode psychosis (stimulant use not excluded)
Similar to individuals with schizophrenia, social cognitive impairments in individuals with a first psychotic episode have been demonstrated. When compared with healthy controls, those with a first episode of psychosis showed significant social cognitive deficits, especially in ToM and emotion recognition52-55. Social cognition was correlated with neurocognition: a lower score in social cognition was associated with greater neurocognitive deficits52,54,56. The relationship between social cognition and social functioning was the focus of 2 studies with divergent conclusions. In a 3 year follow up study55, social cognition did not predict social functioning. In contrast, Stouten et al.56 found that social cognition, when also considering neurocognition and negative symptoms, helped predict some social functioning subdomains such as problems in work, problems in social relationships and problems with self-care. The same study found a strong association between social cognition and impaired social functioning56. When put together, social cognitive biases (such as jumping to conclusion bias, belief inflexibility bias and attention to threat bias), emotion processing speed, general social cognition and attribution and inference bias explained 71% of the variance in social functioning. Although no sex differences were found for social cognition in individuals with a first episode psychosis53, age was identified as a moderator in facial emotion recognition52. This 3-year cohort study found evidence of ToM deficits being a trait of schizophrenia52. ToM deficits in individual with first episode psychosis were unchanged over 3 years despite the treatment delivery. In patients with a first episode of psychosis, social cognition and neurocognition represent two separate areas of vulnerability54. The same study also showed a significant lack of overlap between the different social cognitive measures in terms of results. Given the lack of overlap, it appears important to consider social cognition as a multidimensional construct and not create a global score.
Individuals at ultra-high risk of developing a psychotic disorder (stimulant use not excluded)
A meta-analysis of 19 studies on cognition in patients at ultra high risk of developing a psychotic disorder concluded that despite the significative impairment in social cognition, there was not enough data to support using social cognition to predict the transition to a psychotic disorder57. Of the 19 studies reviewed, social cognition was mentioned in 6 of them, and was the main concept in only 3 studies. The lack of available data on social cognition highlights a gap in the current literature. However, a more recent study58 found that individuals at ultra-high risk who did develop a psychotic disorder showed more emotion recognition deficits than those who didn’t develop a psychotic disorder. According to the study, emotion recognition deficits might be able to predict with a 90% accuracy who will transition to a psychotic disorder.
Individuals with METH use (psychotic symptoms not excluded)
When compared with healthy controls, METH users had lower scores in emotion recognition, especially when they were showed fearful expressions41. Their scores were also lower in two ToM tasks (Hinting task and Reading the mind in the eyes). The relationship between social cognition and dysfunctional personality beliefs was also looked at59. Poor fear recognition was associated with a high level of dysfunctional beliefs. This result can be explained by the hostility bias present in individuals with high levels of dysfunctional beliefs59. There was a positive association between the misclassification of emotions such as disgust and passive-aggressive personality beliefs59.
Discussion
The goal of this scoping review was to describe the literature of the past 20 years on social cognition in METH users with psychosis and psychotic disorder with METH use, with the ultimate goal of informing future studies wishing to differentiate between MIPD and primary psychotic disorders. A plethora of studies have investigated social cognition in people with schizophrenia for instance, with specific deficits being established. Social cognition in METH users is increasingly being studied, also with specific deficits documented (e.g. emotion recognition and ToM)41,35,59-62, although some suggest these deficits might subside with drug cessation9,60. As mentioned earlier, 43% of METH users will experience a MIPD10 and close to 30% of these will be diagnosed with a primary psychotic disorder. Despite the comorbid presentation of psychosis and stimulants use representing more than 20% of the first episode of psychosis population63, and the research endeavour of trying to distinguish MIPD form primary psychotic disorders clinically and cognitively11,31, very few studies have investigated social cognition as a potential domain of interest. Our review found only 17 studies that either included a sample of METH users with psychosis (or did not exclude those with psychotic symptoms) or that included individuals with a psychotic disorder without excluding those who had used METH or other stimulants. The vast majority of studies excluded participants with such comorbid presentations, which brings us to question the ecological validity and the generalizability of their results. Table 2 summarizes the results from this scoping review, and clearly shows the lack of studies on the MIPD population focusing on social cognition. As stated earlier, the selected studies are the one on the schizophrenia population that didn’t excluded METH users and the studies on METH users that didn’t excluded participants with a psychotic disorder. Among those 17 studies, only two looked at the difference between METH users with and without psychosis44,45. Furthermore, the Table illustrates how certain domains of social cognition merit to be studied in METH users, as well as in MIPD. Only two studies, including a meta-analysis, mentioned social knowledge and attributional biases56,57, with a third one mentioning social perception as well46. With deficits in ToM and emotion recognition being the main focus in most studies44,48,49,57, more research is warranted on social knowledge, attributional biases and social perception, as these are also important domains of social cognition. In the literature, studies (that excluded comorbidity profiles) have reported that deficits in social cognition have a considerable impact on social functioning in people with schizophrenia64,65 and in stimulant users66-68. Very few studies have focused on the extent of those deficits in the MIPD population. Some studies have found social functioning deficits in stimulant users with a psychotic disorder69,70 but have not considered the role of social cognition as potentially linked to these social functioning deficits.
Table 2: Scoping Review Findings Classified by Social Cognition Domains and Population
|
|
First Psychosis Disorder, Schizophrenia and Ultra-High Risk
|
METH Users |
METH Users with a History of Psychosis |
|
Theory of Mind |
Ayesa-Arriola et al., 2016; Danaher et al., 2018; Fusar-Poli et al., 2012; Pijnenborg et al., 2013; Schenkel et al., 2005; Simons et al., 2016; Sjølie et al., 2020; Stouten et al., 2017; Van Hooren et al., 2008 |
Hanegraaf et al., 2020 |
|
|
Emotional Processing |
Barkhof et al., 2015; Corcoran et al., 2015; Danaher et al., 2018; Fusar-Poli et al., 2012; Mangelinckx et al., 2017 Simons et al., 2016; Stouten et al., 2017; Vaskinn et al., 2008 |
Hanegraaf et al., 2020; Kim et al., 2011 |
Arunogiri et al., 2019; Uhlmann et al., 2018 |
|
Social Perception |
Barkhof et al., 2015; Fusar-Poli et al., 2012; Stouten et al., 2017 |
|
|
|
Social Knowledge |
Fusar-Poli et al., 2012; Stouten et al., 2017 |
|
|
|
Attributional Bias |
Fusar-Poli et al., 2012; Stouten et al., 2017 |
|
|
In this review, only two studies directly pertained to social cognition in individuals with METH use and psychosis44,45; and none aimed at differentiating MIPD from a primary psychotic disorder. Both studies found that emotion recognition impairments were mostly specific to MIPD, when compared with METH users without psychosis. Those results are in line with several findings on social cognition in individuals with schizophrenia and in METH users as stated earlier. However, Arunogiri’s study44 concluded that the recognition of anger was specially impaired in MIPD but not in individual with METH use without psychosis, whereas Uhlmann’s study45. found that anger recognition was also impaired in METH users without psychosis. The contradiction in these findings reflects the discordance inside this field of study and highlights the need for more research. To the best of our knowledge, no study has yet tried to compare the ToM performance of METH users (with or without psychosis) with those of individuals with a psychotic disorder. More research on ToM is warranted in these populations.
Individual with schizophrenia (stimulant not excluded)
In individuals with schizophrenia, deficits in emotion recognition have clearly been established in this review46,47,51. These findings parallel several other studies done over the years on emotion recognition in schizophrenia71-73. It has been found that individuals with schizophrenia have more difficulties recognising negative than positive emotions46,74-76. Importantly, this deficit appears to be stable over time and presents itself early during the illness73,77. ToM deficits in this review have also clearly been established in individuals with schizophrenia48-50. This finding is consistent with the general literature on ToM as stated in two meta-analyses79-80. ToM was often investigated alongside neurocognition and the correlation between these two concepts has been well established49-50. A recent meta-analysis supports these findings and suggests that ToM is correlated with many different neurocognitive tasks, although the relationship between ToM and specific neurocognitive domains remains unclear81.
Individual with a first episode of psychosis (stimulant use not excluded)
In individuals with first episode of psychosis, deficits in emotion recognition have been established in two studies in this review55,56. However, both studies presented contradictory results. The first study, a 3-year longitudinal study, concluded that social functioning was not associated with social cognition55. However, Stouten et al.56 found the opposite, and most of the literature82-84 suggest that social cognition is a moderator between neurocognition and social functioning. This highlights the need for more research on general and perhaps more specific domains of social cognition in individuals presenting with a first episode of psychosis to reach a conclusion. This review also established the presence of ToM deficit in individuals with a first episode of psychosis52,54,56. A recent meta-analysis (not including substance users) also confirmed those findings85. As in schizophrenia, ToM and neurocognition were often concomitantly investigated, and correlations between ToM and neurocognition have been observed in individuals with a first episode of psychosis52,54,56. Those findings are supported by the current literature in psychosis86-88. ToM has also been identified as a trait in individuals with a first episode of psychosis, particularly in schizophrenia52. While this has been relatively supported by the literature80,89, it is still unclear whether ToM is a trait linked to psychosis or more specifically to schizophrenia85, warranting more research.
Regarding individuals at ultra high-risk for psychosis, deficits in emotion recognition are significantly greater than in those who do not go on to develop a psychotic disorder58. This result is however, not shared with other studies57,90,91. More research on the subject is warranted.
Limitations
A common issue in this domain is the variety of instruments used for the same concept. In this review, more than 10 different tests (standardized and not standardized) were used to assess emotion recognition. The lack of consensus around instruments in social cognition makes the comparison between studies very difficult. A group of experts in social cognition in schizophrenia have attempted at creating a consensus battery92, similar to the MATRICS for neurocognition. Unfortunately, the battery is seldom used with most studies promoting their own battery. This lack of standardized measures was also mentioned in a meta-analysis, where insufficient data on social cognition precluded a definitive conclusion57. The social cognition measures or concepts were often limited or not given enough focus57, with only one or at times two concepts measured49,51,53. Few studies also looked at attributional bias and emotion regulation54,56, whereas most focused on ToM and emotion recognition41,44-53,58.
The foremost limitation of this review is the limited number of studies that met the strict inclusion criteria. By excluding studies that did not include comorbid presentation of psychosis and substance misuse, the number of studies retained was small, limiting the possibility for generalized conclusions. However, the focus of this review was to investigate if social cognition could be used to help differentiate a primary psychotic disorder from a MIPD. Since METH users have a high risk of experiencing MIPD at least once10, it was important to include studies that did not exclude those who had experienced psychosis, therefore, justifying the strictness of our inclusion criteria. Another limitation of our review is the exclusion of studies with a sample under 18 years of age. Close to 20% of first psychotic episodes occur before the age of 1893. METH use sometimes also starts during adolescence94. The exclusion of this population could have led to fewer articles regarding social cognition and the onset of those disorders. Nonetheless, few studies in early psychosis with adolescence have been conducted95-97, suggesting that a limited number of studies would have possibly been added.
Recommendations
Based on the findings in this review, we recommend the following for future research:
- Compare social cognition in METH users with and without psychosis.
- Compare social cognition in people with schizophrenia with and without stimulant use / misuse.
- Include multiple domains of social cognitions in studies (social perception, social knowledge and attributional bias), and not only on emotional processing and ToM.
- Determine the predictive value of social cognition, alongside other potential variables, such as negative symptoms, visual memory/cognitive deficits, or visual hallucinations, in order to develop a brief assessment battery that would allow to distinguish MIPD from a primary psychotic disorder like schizophrenia, at first hospitalization for meth-related psychosis.
To our knowledge, this is the first scoping review aiming to evaluate if social cognition could be used to differentiate a first episode psychosis from MIPD. Our results confirm that social cognition impairments are well established in individuals with a psychotic disorder, such as schizophrenia, and preliminary results have also been found in METH users. This review suggests that social cognition warrants future investigations as a potential domain to help differentiate a first episode of a primary psychosis from MIPD. This scoping review highlighted a significant gap in the literature, as no study has yet used social cognition to compare both diagnoses.
References:
- United nations office on drugs and crime (UNODC). World drug report. 2015. https://www.unodc.org/documents/wdr2015/World_Drug_Report_2015.pdf [Accessed October 15, 2020].
- Twillman RK, Dawson E, LaRue L, et al. Evaluation of Trends of Near-Real-Time Urine Drug Test Results for Methamphetamine, Cocaine, Heroin, and Fentanyl. JAMA Network Open. 2020;3(1): DOI:10.1001/jamanetworkopen.2019.18514.
- Sommers I, Baskin D, Baskin-Sommers A. Methamphetamine use among young adults: Health and social consequences. Addictive Behaviors. 2006;31(8):1469-1476. https://doi.org/10.1016/j.addbeh.2005.10.004
- Won S, Hong RA, Shohet RV, et al. Methamphetamineâassociated cardiomyopathy. Clinical cardiology. 2013;36(12):737-742. doi: 10.1002/clc.22195.
- Moszczynska A, Callan SP. Molecular, Behavioral, and Physiological Consequences of Methamphetamine Neurotoxicity: Implications for Treatment. The journal of pharmacology and experimental therapeutics. 2017;362:474-488. DOI: https://doi.org/10.1124/jpet.116.238501.
- Anglin MD, Burke C, Perrochet B, et al. History of the methamphetamine problem. Journal of psychoactive drugs. 2000;32(2):137-141. DOI: 10.1080/02791072.2000.10400221.
- Cho AK, Melega WP. Patterns of Methamphetamine Abuse and Their Consequences. Journal of Addictive Diseases. 2001;21(1):21-34. DOI: 10.1300/J069v21n01_03.
- Marshall JF, et O’Dell SJ. Methamphetamine influences on brain and behavior: unsafe at any speed. Trends in Neurosciences. 2012;35(9):536-545. DOI: http://dx.doi.org/10.1016/j.tins.2012.05.006.
- Zhong N, Jiang H, Du J, et al. The cognitive impairments and psychological wellbeing of methamphetamine dependent patients compared with health controls. Progress in Neuro-Psychopharmacology & Biological Psychiatry. 2016;69:31-37. DOI: http://dx.doi.org/10.1016/j.pnpbp.2016.04.005.
- Lecomte T, Dumais A, Dugré JR, et al. The prevalence of substance-induced psychotic disorder in methamphetamine misusers: A meta-analysis. Psychiatry Research. 2018;268:189-192. DOI: https://doi.org/10.1016/j.psychres.2018.05.033.
- Wearne TA, Cornish JL. A Comparison of Methamphetamine-Induced Psychosis and Schizophrenia: A Review of Positive, Negative, and Cognitive Symptomatology. Frontiers in Psychiatry. 2018;9(491):1-21. DOI: 10.3389/fpsyt.2018.00491.
- McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first-episode psychosis in a clinical sample with subthreshold symptoms. Archives of general psychiatry. 2002;59(10):921-928. doi:10.1001/archpsyc.59.10.921.
- Rössler W, Salize HJ, van Os J, et al. Size of burden of schizophrenia and psychotic disorders. European Neuropsychopharmacology. 2005; 15: 399-409. doi:10.1016/j.euroneuro.2005.04.009.
- Arciniegas DB. Psychosis. Behavioral Neurology and Neuropsychiatry. 2015;21(3):715-736. DOI: 10.1212/01.CON.0000466662.89908.e7.
- Smout MF, Longo M, Harrison S, et al. Psychosocial treatment for methamphetamine use disorders: A preliminary randomized controlled trial of cognitive behavior therapy and acceptance and commitment therapy. 2013;(pp. 104-113). Routledge.
- Sullivan SA, Carroll R, Peters TJ, et al. Duration of untreated psychosis and clinical outcomes of first episode psychosis: an observational and an instrumental variables analysis. Early Intervention in Psychiatry. 2019;13(4):841-847. https://doi.org/10.1111/eip.12676.
- Hui CL, Honer WG, Lee EH, et al. Long-term effects of discontinuation from antipsychotic maintenance following first-episode schizophrenia and related disorders: a 10 year follow-up of a randomised, double-blind trial. The Lancet Psychiatry. 2018;5(5):432-442.
- Emsley R, Chiliza B, Asmal L, et al. The nature of relapse in schizophrenia. BMC psychiatry. 2013;13(1):1-8.
- Iyer SN, Malla AK. Intervention précoce pour la psychose: concepts, connaissances actuelles et orientations futures. Santé mentale au Québec. 2014;39(2):201–229. https://doi.org/10.7202/1027840ar.
- Cheung D, Roper L, Purdon SE. Pathways to (specialized) care: patient costs and contacts en route to a first-episode psychosis clinic. Early Intervention in Psychiatry. 2013;8:375-381. doi:10.1111/eip.12093.
- Glasner-Edwards S, Mooney LJ. Methamphetamine Psychosis: Epidemiology and Management. Therapy in practice. 2014;28: 1115-1126. DOI 10.1007/s40263-014-0209-8.
- McKetin R, McLaren J, Lubman DI, et al. The prevalence of psychotic symptoms among methamphetamine users. Research report. 2006;101(10). DOI: https://doi.org/10.1111/j.1360-0443.2006.01496.x.
- Srisurapanont M, Ali R, Marsden J, et al. Psychotic symptoms in methamphetamine psychotic in-patients. International Journal of Neuropsychopharmacology. 2003;6(4):347-352. DOI: https://doi.org/10.1017/S1461145703003675.
- Kurihara T, Kato M, Reverger R, et al. Seventeen-year clinical outcome of schizophrenia in Bali. European Psychiatry. 2011;26:333-338. DOI: doi:10.1016/j.eurpsy.2011.04.003.
- Tan S, Liu D. A review of the Chinese literature on cognitive remediation in psychosis. Asian Journal of Psychiatry. 2016;22:129-134. DOI: http://dx.doi.org/10.1016/j.ajp.2016.06.012.
- Veling W, Selten JP, Mackenbach JP, et al. Symptoms at first contact for psychotic disorder: Comparison between native Dutch and ethnic minorities. Schizophrenia Research. 2007;95:30-38. DOI: doi:10.1016/j.schres.2007.06.024.
- Shelly J, Uhlmann A, Sinclair H, et al. First-rank symptoms in methamphetamine psychosis and schizophrenia. Psychopathology. 2016;49(6):429-435. https://doi.org/10.1159/000452476.
- McKetin R, Baker AL, Dawe S, et al. Differences in the symptom profile of methamphetamine-related psychosis and primary psychotic disorders. Psychiatry research. 2017;251:349-354. https://doi.org/10.1016/j.psychres.2017.02.028.
- Bramness JG, Gundersen OH, Guterstam J, et al. Amphetamine-induced psychosis - a separate diagnostic entity or primary psychosis triggered in the vulnerable? BMC Psychiatry. 2012;12(1):221. DOI: https://doi.org/10.1186/1471-244X-12-221.
- Kalkstein S, Hurford I, Gur RC. Neurocognition in schizophrenia. In Behavioral neurobiology of schizophrenia and its treatment. 2010;4:373-390. DOI: https://doi.org/10.1007/7854_2010_42.
- MihaljeviÄ-Peleš A, JanoviÄ MB, Šagud M, et al. Cognitive deficit in schizophrenia: an overview. Psychiatria Danubina. 2019;31(2):139-142.
- Bora E, Murray RM. Meta-analysis of cognitive deficits in ultra-high risk to psychosis and first-episode psychosis: do the cognitive deficits progress over, or after, the onset of psychosis?. Schizophrenia bulletin. 2014;40(4):744-755. DOI:https://doi.org/10.1093/schbul/sbt085.
- Bora E, Pantelis C. Meta-analysis of cognitive impairment in first-episode bipolar disorder: comparison with first-episode schizophrenia and healthy controls. Schizophrenia bulletin. 2015;41(5):1095-1104. DOI:https://doi.org/10.1093/schbul/sbu198.
- Bouchard V, Lecomte T, Mueser KT. Could cognitive deficits help distinguish methamphetamine-induced psychosis from a psychotic disorder with substance abuse? Mental Health and Substance Use. 2013;6(2):101-110. DOI: https://doi.org/10.1080/17523281.2012.693522.
- Potvin S, Pelletier J, Grot S, et al. Cognitive deficits in individuals with methamphetamine use disorder: A meta-analysis. Addictive behaviors. 2018;80:154-160. DOI: https://doi.org/10.1016/j.addbeh.2018.01.021.
- Basterfield C, Hester R, Bowden SC. A meta-analysis of the relationship between abstinence and neuropsychological functioning in methamphetamine use disorder. Neuropsychology. 2019;33(5):739–753. https://doi.org/10.1037/neu0000552.
- Hall MG, Hauson AO, Wollman SC, et al. Neuropsychological comparisons of cocaine versus methamphetamine users: A research synthesis and meta-analysis. The American Journal of Drug and Alcohol Abuse. 2017;44(3):277–293. DOI: 10.1080/00952990.2017.1355919.
- Scott JC, Woods SP, Matt GE, et al. Neurocognitive Effects of Methamphetamine: A Critical Review and Meta-analysis. Neuropsychology Review. 2007;17(3):275–297. doi:10.1007/s11065-007-9031-0.
- De Jaegher H, Di Paolo E, Gallagher S. Can social interaction constitute social cognition?. Trends in cognitive sciences. 2010;14(10):441-447. DOI: https://doi.org/10.1016/j.tics.2010.06.009.
- Kitchen H, Rofail D, Heron L, et al. Cognitive impairment associated with schizophrenia: a review of the humanistic burden. Advances in therapy. 2012;29(2):148-162. DOI 10.1007/s12325-012-0001-4.
- Kim YT, Kwon DH, Chang Y. Impairments of facial emotion recognition and theory of mind in methamphetamine abusers. Psychiatry Research. 2011;186(1):80-84. DOI: https://doi.org/10.1016/j.psychres.2010.06.027.
- Peters MD, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. JBI Evidence Implementation. 2015;13(3):141-146. doi: 10.1097/XEB.0000000000000050.
- Arksey H, O'Malley L. (2005). Scoping studies: towards a methodological framework. International journal of social research methodology. 2005;8(1):19-32. https://doi.org/10.1080/1364557032000119616.
- Arunogiri S, Verdejo-Garcia A, McKetin R, et al. Emotion Recognition and Impulsive Choice in Relation to Methamphetamine Use and Psychosis Symptoms. Frontiers in Psychiatry. 2019;10. DOI: 10.3389/fpsyt.2019.00889.
- Uhlmann A, Ipser JC, Wilson D, et al. Social cognition and aggression in methamphetamine dependence with and without a history of psychosis. Metabolic brain disease. 2018;33(2):559-568. DOI: https://dx.doi.org/10.1007/s11011-017-0157-3.
- Barkhof E, de Sonneville LM, Meijer CJ, et al. Specificity of facial emotion recognition impairments in patients with multi-episode schizophrenia. Schizophrenia Research: Cognition. 2015;2(1):12-19. DOI: https://doi.org/10.1016/j.scog.2015.01.001.
- Mangelinckx C, Belge JB, Maurage P, et al. Impaired facial and vocal emotion decoding in schizophrenia is underpinned by basic perceptivo-motor deficits. Cognitive Neuropsychiatry. 2017;22(6):461-467. DOI: http://dx.doi.org/10.1080/13546805.2017.1382342.
- Pijnenborg GHM, Spikman JM, Jeronimus BF, et al. Insight in schizophrenia: associations with empathy. European Archives of Psychiatry and Clinical Neuroscience. 2013;263(4):299-307. DOI: 10.1007/s00406-012-0373-0.
- Schenkel LS, Spaulding WD, Silverstein SM. Poor premorbid social functioning and theory of mind deficit in schizophrenia: evidence of reduced context processing? Journal of psychiatric research. 2005;39(5):499-508. DOI: https://doi.org/10.1016/j.jpsychires.2005.01.001.
- Sjølie C, Meyn EK, Raudeberg R, et al. Nonsocial cognitive underpinnings of theory of mind in schizophrenia. Psychiatry Research. 2020;113055. DOI: https://doi.org/10.1016/j.psychres.2020.113055.
- Vaskinn A, Sundet K, Friis S, et al. Emotion perception and learning potential: mediators between neurocognition and social problem-solving in schizophrenia? Journal of the International Neuropsychological Society. 2008;14(2):279-288. DOI: https://doi.org/10.1017/S1355617708080314.
- Ayesa-Arriola R, Setién-Suero E, Neergaard KD, et al. Evidence for trait related theory of mind impairment in first episode psychosis patients and its relationship with processing speed: a 3 year follow-up study. Frontiers in psychology. 2016;7: 592. DOI: https://doi.org/10.3389/fpsyg.2016.00592.
- Danaher H, Allott K, Killackey E, et al. An examination of sex differences in neurocognition and social cognition in first-episode psychosis. Psychiatry Research. 2018;259:36-43. DOI: https://doi.org/10.1016/j.psychres.2017.09.053.
- Van Hooren S, Versmissen D, Janssen I, et al. Social cognition and neurocognition as independent domains in psychosis. Schizophrenia Research. 2008;103(1-3):257-265. DOI: https://doi.org/10.1016/j.schres.2008.02.022.
- Simons CJ, Bartels-Velthuis AA, Pijnenborg GH, Genetic Risk and Outcome of Psychosis (GROUP) Investigators. Cognitive performance and long-term social functioning in psychotic disorder: a three-year follow-up study. PloS one. 2016;11(4):e0151299. DOI: https://doi.org/10.1371/journal.pone.0151299.
- Stouten LH, Veling W, Laan W, et al. Psychosocial functioning in firstâepisode psychosis and associations with neurocognition, social cognition, psychotic and affective symptoms. Early Intervention in Psychiatry. 2017;11(1):23-36. DOI: https://doi.org/10.1111/eip.12210.
- Fusar-Poli P, Deste G, Smieskova R, et al. Cognitive functioning in prodromal psychosis: a meta-analysis. Archives of general psychiatry. 2012;69(6):562-571. DOI:10.1001/archgenpsychiatry.2011.1592.
- Corcoran CM, Keilp JG, Kayser J, et al. Emotion recognition deficits as predictors of transition in individuals at clinical high risk for schizophrenia: a neurodevelopmental perspective. Psychological medicine. 2015;45(14):2959. DOI: doi: 10.1017/S0033291715000902.
- Hanegraaf L, Arunogiri S, Hohwy J, et al. Dysfunctional personality beliefs and emotion recognition in individuals with methamphetamine dependence. Addictive Behaviors. 2020;105:106336. DOI: https://doi.org/10.1016/j.addbeh.2020.106336.
- Henry JD, Mazur M, Rendell PG. Socialâcognitive difficulties in former users of methamphetamine. British Journal of Clinical Psychology. 2009;48(3):323-327. DOI: https://doi.org/10.1111/j.2044-8260.2009.tb00487.x.
- Homer BD, Solomon TM, Moeller RW, et al. Methamphetamine abuse and impairment of social functioning: A review of the underlying neurophysiological causes and behavioral implications. Psychological Bulletin. 2008;134(2):301-310. doi:10.1037/0033-2909.134.2.301.
- Quednow BB. Social cognition and interaction in stimulant use disorders. Current opinion in behavioral sciences. 2017;13:55-62. DOI:https://doi.org/10.1016/j.cobeha.2016.10.001
- Abdel-Baki A, Ouellet-Plamondon C, Salvat É, et al. Symptomatic and functional outcomes of substance use disorder persistence 2 years after admission to a first-episode psychosis program. Psychiatry research. 2017;247:113-119. DOI: https://doi.org/10.1016/j.psychres.2016.11.007
- Harvey PD, Penn D. Social cognition: the key factor predicting social outcome in people with schizophrenia?. Psychiatry (Edgmont). 2010;7(2):41.
- Veltro F, Mazza M, Vendittelli N, et al. A comparison of the effectiveness of problem solving training and of cognitive-emotional rehabilitation on neurocognition, social cognition and social functioning in people with schizophrenia. Clinical practice and epidemiology in mental health: CP & EMH. 2011;7:123. doi: 10.2174/1745017901107010123.
- Preller KH, Herdener M, Schilbach L, et al. Functional changes of the reward system underlie blunted response to social gaze in cocaine users. Proceedings of the National Academy of Sciences. 2014;111(7):2842-2847. https://doi.org/10.1073/pnas.1317090111.
- Quednow BB. The rise of the ego: social cognition and interaction in cocaine users. In Neuropathology Of Drug Addictions And Substance Misuse (pp. 257-268). Academic Press. 2016. https://doi.org/10.1016/B978-0-12-800212-4.00025-X.
- Kroll SL, Wunderli MD, Vonmoos M, et al. Socio-cognitive functioning in stimulant polysubstance users. Drug and alcohol dependence. 2018;190:94-103. https://doi.org/10.1016/j.drugalcdep.2018.06.001.
- Ouellet-Plamondon C, Abdel-Baki A, Salvat É, et al. Specific impact of stimulant, alcohol and cannabis use disorders on first-episode psychosis: 2-year functional and symptomatic outcomes. Psychological Medicine. 2017;47(14):2461-2471.
- Cantwell R. Substance use and schizophrenia: effects on symptoms, social functioning and service use. The British Journal of Psychiatry. 2003;182(4):324-329.
- De Jong JJ, Hodiamont PPG, Van den Stock J, et al. Audiovisual emotion recognition in schizophrenia: reduced integration of facial and vocal affect. Schizophrenia research. 2009;107(2-3):286-293. https://doi.org/10.1016/j.schres.2008.10.001
- Fernandez-Modamio M, Gil-Sanz D, Arrieta-Rodriguez M, et al. Emotion recognition in patients with schizophrenia: The role of sex. Psicothema. 2020;32(2):197-203. doi: 10.7334/psicothema2019.310.
- Penn DL, Combs DR, Ritchie M, et al. Emotion recognition in schizophrenia: Further investigation of generalized versus specific deficit models. Journal of Abnormal Psychology. 2000;109(3):512–516. https://doi.org/10.1037/0021-843X.109.3.512
- Baez S, Herrera E, Villarin L, et al. Contextual social cognition impairments in schizophrenia and bipolar disorder. PloS one. 2013;8(3):e57664. DOI: https://doi.org/10.1371/journal.pone.0057664.
- Daros AR, Ruocco AC, Reilly JL,et al. Facial emotion recognition in first-episode schizophrenia and bipolar disorder with psychosis. Schizophrenia research. 2014;153(1-3):32-37. DOI: https://doi.org/10.1016/j.schres.2014.01.009.
- Goghari VM, Sponheim SR. More pronounced deficits in facial emotion recognition for schizophrenia than bipolar disorder. Comprehensive psychiatry. 2013;54(4):388-397. DOI: https://doi.org/10.1016/j.comppsych.2012.10.012.
- Amminger GP, Schäfer MR, Klier CM, et al. Facial and vocal affect perception in people at ultraâhigh risk of psychosis, firstâepisode schizophrenia and healthy controls. Early Intervention in Psychiatry. 2012;6(4):450-454. DOI: https://doi.org/10.1111/j.1751-7893.2012.00362.x.
- Penn DL, Sanna LJ, Roberts DL. Social cognition in schizophrenia: an overview. Schizophrenia bulletin. 2008;34(3):408-411. DOI: https://doi.org/10.1093/schbul/sbn014.
- Bora E, Yucel M, Pantelis C. Theory of mind impairment in schizophrenia: meta-analysis. Schizophrenia research. 2009;109(1-3):1-9. DOI: https://doi.org/10.1016/j.schres.2008.12.020.
- Sprong M, Schothorst P, Vos E, et al. Theory of mind in schizophrenia: meta-analysis. The British Journal of Psychiatry. 2007;191(1):5-13. DOI: https://doi.org/10.1192/bjp.bp.107.035899.
- Thibaudeau É, Achim AM, Parent C, et al. A meta-analysis of the associations between theory of mind and neurocognition in schizophrenia. Schizophrenia research. 2020;216:118-128. DOI: https://doi.org/10.1016/j.schres.2019.12.017.
- Addington J, Saeedi H, Addington D. Facial affect recognition: a mediator between cognitive and social functioning in psychosis?. Schizophrenia research. 2006;85(1-3):142-150. DOI: https://doi.org/10.1016/j.schres.2006.03.028.
- Addington J, Saeedi H, Addington D. Influence of social perception and social knowledge on cognitive and social functioning in early psychosis. The British Journal of Psychiatry. 2006;189(4):373-378. DOI: https://doi.org/10.1192/bjp.bp.105.021022.
- Jaramillo P, Fuentes-Durá I, Ruiz JC. Cognition, social cognition and social functioning in schizophrenia. Psychology, Society, & Education. 2009;1(1):13-24.
- Bora E, Pantelis C. Theory of mind impairments in first-episode psychosis, individuals at ultra-high risk for psychosis and in first-degree relatives of schizophrenia: systematic review and meta-analysis. Schizophrenia research. 2013;144(1-3):31-36. https://doi.org/10.1016/j.schres.2012.12.013
- Koelkebeck K, Pedersen A, Suslow T, et al. Theory of Mind in first-episode schizophrenia patients: correlations with cognition and personality traits. Schizophrenia research. 2010;119(1-3):115-123. DOI: https://doi.org/10.1016/j.schres.2009.12.015.
- Mazza M, Pollice R, Pacitti F, et al. New evidence in theory of mind deficits in subjects with chronic schizophrenia and first episode: correlation with symptoms, neurocognition and social function. Rivista di psichiatria. 2012;47(4):327-336. DOI: 10.1708/1139.12561.
- Catalan A, Angosto V, Díaz A, et al. The relationship between theory of mind deficits and neurocognition in first episode-psychosis. Psychiatry Research. 2018;268:361-367. DOI: https://doi.org/10.1016/j.psychres.2018.06.066
- Janssen I, Krabbendam L, Jolles J, et al. Alterations in theory of mind in patients with schizophrenia and nonâpsychotic relatives. Acta Psychiatrica Scandinavica. 2003;108(2):110-117. DOI: https://doi.org/10.1034/j.1600-0447.2003.00092.x
- Thompson AD, Bartholomeusz C, Yung AR. Social cognition deficits and the ‘ultra high risk’for psychosis population: a review of literature. Early intervention in psychiatry. 2011;5(3):192-202. DOI: https://doi.org/10.1111/j.1751-7893.2011.00275.x.
- Van Donkersgoed RJM, Wunderink L, Nieboer R, et al. Social cognition in individuals at ultra-high risk for psychosis: a meta-analysis. PloS one. 2015;10(10). DOI: https://doi.org/10.1371/journal.pone.0141075.
- Pinkham AE, Penn DL, Green MF, et al. The social cognition psychometric evaluation study: results of the expert survey and RAND panel. Schizophrenia bulletin. 2014;40(4):813-823. DOI: https://doi.org/10.1093/schbul/sbt081.
- Ballageer T, Malla A, Manchanda R, et al. Is adolescent-onset first-episode psychosis different from adult onset? Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44(8):782-789. DOI: 10.1097/01.chi.0000164591.55942.ea.
- Cservenka A, Ray LA. Self-reported attentional and motor impulsivity are related to age at first methamphetamine use. Addictive behaviors. 2017;65:7-12. DOI: https://doi.org/10.1016/j.addbeh.2016.09.008.
- Horton LE, Tarbox SI, Olino TM, et al. Trajectories of premorbid childhood and adolescent functioning in schizophrenia-spectrum psychoses: a first-episode study. Psychiatry research. 2015;227(2-3):339-346. DOI: https://doi.org/10.1016/j.psychres.2015.02.013.
- McClellan J, Stock S. Practice parameter for the assessment and treatment of children and adolescents with schizophrenia. Journal of the American Academy of Child & Adolescent Psychiatry. 2013;52(9):976-990. DOI: https://doi.org/10.1016/j.jaac.2013.02.008.
- Reichert A, Kreiker S, Mehler-Wex C, et al. The psychopathological and psychosocial outcome of early-onset schizophrenia: Preliminary data of a 13-year follow-up. Child and Adolescent Psychiatry and Mental Health. 2008;2(6). DOI: https://doi.org/10.1186/1753-2000-2-6.