
Body Composition Changes in Psychiatric Patients Treated with Lithium and Valproate
Seyed-Shahab Banihashem1, Sahar Ashrafzadeh2, Mehrshad Poursaied Esfahani3, Zeinab Morsalivachin4, Alireza Shamsi5, Somaye Motazedian6, Mohammadreza Mousavipour7*
1Department of Psychosomatic Medicine, Taleghani Hospital Research Development Committee, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2David Geffen School of Medicine, University of California, Los Angeles, CA, USA
3Department of Sports and Exercise Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4Department of Surgery School of Medicine, Iran University of Medical Sciences. Tehran, Iran
5Shahid Beheshti University of Medical Sciences, Taleghani Hospital
6Taleghani Hospital, Department of Psychosomatic Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
7School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Purpose: To compare the effects of lithium and valproate on the body composition of psychiatric patients.
Methods: This prospective cohort study evaluated the effects of lithium and valproate on body composition. Twenty-eight patients with type I bipolar disorder aged 23-54 years who just had started monotherapy were recruited. Body weight, percent body fat (PBF), soft lean mass, body mass index (BMI), and total body water were measured at baseline, one month, and six months. Changes in the body composition parameters between patients taking lithium (n=14) versus valproate (n=14) were compared.
Findings: Overall mean age of study participants was 37.21 (±8) years, and 53.5% of patients were female. Average body weight gains in the first month were 1.3 kg and 2.2 kg for the lithium and valproate groups, respectively (p-value = 0.042). Mean body weight gain in the six months compared to the baseline was only 0.6 kg for the lithium group, while it was 4.3 kg for the valproate group (p-value < 0.001). The average increase in PBF at six months among patients treated with lithium versus valproate was 0.07% versus 2.2% respectively (p-value = 0.018). Patients treated with lithium had a smaller increase in their BMI in the sixth month of the study compared to the valproate group, with a mean change of 0.2 versus 2.3 kg/m2, respectively (p-value = 0.019).
Conclusions: Our findings suggest that in patients with type I bipolar disorder, valproate leads to greater weight gain, BMI, and increase in PBF compared to lithium.
Introduction
Mental disorders are sometimes associated with physical signs and symptoms. Intensive change in body composition is one of the physical signs of mental disorders that might be due to the related treatments or changes in diet and overall lifestyle of patients suffering from mental disorders1,2. Abrupt changes in body composition can lead to worsening clinical outcomes and may affect on mood and self-esteem and consequently can affect the quality of life of patients3. Therefore, drastic weight alterations must be considered in patients’ medications and treatment regimens, particularly in chronic diseases such as mental disorders that require long-term treatment3.
Mental disorders are a prevalent global health challenge, and rates of mental illness are growing worldwide1. Different therapeutic approaches have been developed in recent years. Lithium is known as the standard treatment for mood stabilization, and the high efficacy of this treatment has been proven in multiple studies4,5. However, similar to most other medications, several adverse effects have been reported for lithium. There is evidence indicating a strong association between lithium use and changes in anthropometric indexes including increased body weight and body mass index (BMI)6,7,8. Increasing body weight may lead to further complications such as cardiovascular disease, diabetes mellitus, and metabolic syndrome, and it additionally may impose high costs on patients and health care systems9. Therefore, the potential adverse effect must be fully considered in the management of patients.
Gaining weight in patients with a mental disorder is a multifactorial phenomenon. Genetic predisposition, drugs, lifestyle, and behavioral and environmental factors are known factors that contribute to increasing body weight in psychiatric patients. However, the underlying pharmacological mechanism is still unclear10. As mentioned previously, psychotropic medications such as lithium are one of the culprits for weight gain in this patient population. Some studies have reported from 2 to 4.2 kg increase in average body weight among lithium-treated patients over a period of one year11,12. The same adverse effect has also been reported for another mood stabilizer, sodium valproate8. The possible underlying mechanism for such a weight gain may be serotonin accumulation in the central nervous system. This can induce a false appetite, low physical activity, and change in dietary behaviors, ultimately increasing body weight13,14.
The burden of mental disorders is drastically growing in both developed and developing countries, and introducing effective therapeutic approaches with the least side effects is a highly sought after but challenging responsibility of psychiatrists1. However, few studies have evaluated the effectiveness and safety of different mood stabilizers in patients with mental disorders. The current study aimed to compare the effects of lithium and sodium valproate on various body composition parameters among psychiatric patients with bipolar I disorder.
Material and Methods
Patients
We carried out an observational prospective cohort study on 28 patients referred from psychiatric outpatient clinics of Taleghani Hospital over a six-month period from 2019 to 2020 in Tehran, Iran. All the patients included in this study were over 18 years old, had type I bipolar disorder, and were in the maintenance phase of their treatment. Patients had recently been prescribed to take a monotherapy of either lithium or sodium valproate before being referred to our center. The dosage was between 600 to 1200 milligrams for lithium and 400 to 1200 milligrams for valproate. Women who were either pregnant or intended to get pregnant, and patients taking medications affecting their body weight (other than lithium and valproate) were excluded from the study. Other exclusion criteria included having a disease that could affect body weight; long-term hospitalization; suffering from severe distress (that may alter the body weight, physical activity, and diet); experiencing a considerable change in routine diet; change in physical activity; and having a prior history of non-compliance with prescribed medications. The study protocol was explained to participants before they signed informed consent forms.
Ethics Approval
The current study was reviewed and approved by Research Ethics Committee at Shahid Beheshti University of Medical Sciences (IR.SBMU.MSP.REC.1389.144).
Pharmacotherapy and Outcome Measurement
Study participants were selected from patients who had not received lithium or valproate for at least the previous six months and had just been started on monotherapy of either lithium or valproate before being referred to our center. Both groups (n=14 each) of either lithium or valproate therapy underwent evaluation by using bioelectric impedance analysis (BIA) in the morning while fasting at the study’s baseline and the ensuing one month and six months after the treatment started. The body composition indexes measured included the participants’ body mass index (BMI), percentage of body fat (PBF), total body water (TBW), and soft lean mass (SLM). The BIA machine used was (GAIA 359) JAWON PLUS.
Statistical Analysis
Descriptive statistics were applied to describe both demographic and clinical characteristics of the study participants. Within groups, differences were assessed by using repeated-measure ANOVA. The mean changes in the investigated outcomes were calculated by subtracting the values in the first and sixth months from the baselines, and then an independent T-test compared the mean change in the first and sixth months of the study between groups. All statistical analyses were performed at α 2-tailed level of 0.05 using Stata software (Version 14.1, College Station, Texas, USA).
Results
The study included 28 patients referred from outpatient psychiatry clinics to our center. The overall mean age (±SD) of study participants was 37.21 (±8.12) years, and 53.5% of patients were female. The baseline average body weight, PBF, SLM, BMI, and TBW for all of the patients participating in this study were 74.20 (±17) kg, 26.27 (±9), 50.04 (±11.4), 25.80 (±5.6) kg/m2, and 39.10 (±8.8), respectively. At baseline, there were no statistically significant differences in body composition indexes between the two groups (p-value > 0.05) (Table 1).
Table 1: Baseline characteristics of study participants
|
Characteristics |
Total (n=28) |
Lithium (n=14) |
Valproate (n=14) |
P-value |
|
Female gender, n (%) |
15 (53.5%) |
8 (57.10%) |
7 (50.00%) |
0.705 |
|
Age, Mean (±SD) (year) |
37.21 (±8.12) |
36.79 (9.07) |
37.64 (±7.38) |
0.786 |
|
Weight, Mean (±SD) (kg) |
74.20 (±16.65) |
73.47 (±16.77) |
74.92 (±17.14) |
0.824 |
|
PBF, Mean (±SD)a |
26.27 (±9.04) |
26.24 (±9.25) |
26.30 (±9.17) |
0.985 |
|
SLM, Mean (±SD)b |
50.04 (±11.38) |
49.78 (±12.29) |
50.31 (±10.85) |
0.906 |
|
BMI, Mean (±SD) (kg/m2)c |
25.80 (±5.62) |
25.70 (±6.37) |
25.89 (±5.00) |
0.932 |
|
TBW, Mean (±SD)d |
39.10 (±8.76) |
38.90 (±9.42) |
39.30 (±8.39) |
0.905 |
p-value less than 5% is considered significant.
a PBF: percent body fat
b SLM: soft lean mass
c BMI: body mass index
d TBW: total body water
Table 2 compared the trend of body composition index characteristics over the study within each group. There were no significant changes in body composition indices in the lithium group. A slight increase in the investigated variables were noted between the first and sixth month of the study; however, these changes did not reach statistical significance.
However, among the valproate group, the average body weight increased from 74.92 (±17) kg at baseline to 77.19 (±17) in the first month and 79.22 (±16) in the sixth month, which was statistically significant (p-value = 0.016). The same statistically significant (p-value = 0.016) upward trend was also found for PBF in the valproate group, where it was 26.3 at baseline and continuously increased and reached a peak in the sixth month (mean PBF of 28.59 ±9.5 at six months). Although all other investigated variables, including SLM, BMI, and TBW, had increased in the valproate group over the study period, there were no statistically significant differences over time (p-value > 0.05) (Table 2).
Table 2: Study participants’ body composition characteristics at three distinctive times over the study period
|
|
Lithium (n=14) |
Valproate (n=14) |
||||||
|
Characteristics |
Baseline |
1st Month |
6th Month |
P-value |
Baseline |
1st Month |
6th Month |
P-value |
|
Weight, Mean (±SD) kg |
73.47±16 |
74.78±16 |
74.12±16 |
0.240 |
74.92±17 |
77.19±17 |
79.22±16 |
0.016* |
|
PBF, Mean (±SD)a |
26.24±9 |
27.02±8 |
26.31±9 |
0.433 |
26.30±9 |
27.50±9 |
28.59±9 |
0.011* |
|
SLM, Mean (±SD)b |
49.78±12 |
50.48±11 |
50.13±11 |
0.584 |
50.31±10 |
50.98±10 |
51.64±9 |
0.137 |
|
BMI, Mean (±SD) kg/m2c |
25.70±6 |
26.22±6 |
25.96±6 |
0.251 |
25.89±5 |
27.45±5 |
28.27±5 |
0.439 |
|
TBW, Mean (±SD)d |
38.90±9 |
39.37±9 |
39.05±8 |
0.522 |
39.30±8 |
39.79±8 |
40.25±7 |
0.167 |
*p-value less than 5% is considered significant.
a PBF: percent body fat
b SLM: soft lean mass
c BMI: body mass index
d TBW: total body water
Additionally, the mean change of body composition indexes between the lithium and valproate groups in the first and sixth months of the study were compared. The average body weight increase in the first month was 1.3 and 2.2 kg for the lithium and valproate groups, respectively, and the observed difference was statistically significant. The mean increase in body weight between the first month and the sixth month for the valproate group was 4.3 kg, while it was only 0.6 in the lithium group compared to the baseline (p-value < 0.001). The average increase in PBF among patients treated with lithium was 0.07 in the sixth month of the study, whereas it was 2.2 in those patients who received valproate (p-value = 0.108). There was a greater mean change in BMI between the first and the sixth months of the study in the valproate group (mean change = 2.3 kg/m2) compared to the lithium group (mean change = 0.2) (p-value = 0.019) (Table 3). As Figures 1 to 3 present, lithium increased weight gain in the 1st month, and then body weight started to decrease again within the six-month period.
Table 3: Comparison of changes in body composition indexes between patients who received lithium versus valproate after one month and six months (n=28)
|
|
Wight (kg) |
PBFa |
SLMb |
BMI (kg/m2)c |
TBWd |
|||||
|
Time Point |
Lithium |
Valproate |
Lithium |
Valproate |
Lithium |
Valproate |
Lithium |
Valproate |
Lithium |
Valproate |
|
1st Month |
1.3 (1.1) |
2.2 (1.1) |
0.7 (1.3) |
1.2 (0.7) |
0.7 (0.9) |
0.6 (0.8) |
0.5 |
1.5 |
0.4 (0.5) |
0.4 (0.5) |
|
P-value |
0.042* |
0.340 |
0.948 |
0.171 |
0.941 |
|||||
|
6th Month |
0.6 (1.6) |
4.3 (2.6) |
0.07 (3.0) |
2.2 (1.2) |
0.3 (2.1) |
1.3 (1.3) |
0.2 (0.6) |
2.3 (2.8) |
0.1 (1.7) |
0.9 (1.0) |
|
P-value |
<0.001* |
0.018* |
0.163 |
0.019* |
0.161 |
|||||
*p-value less than 5% is considered significant.
The numbers in parentheses show the standard deviations.
a PBF: percent body fat
b SLM: soft lean mass
c BMI: body mass index
d TBW: total body water
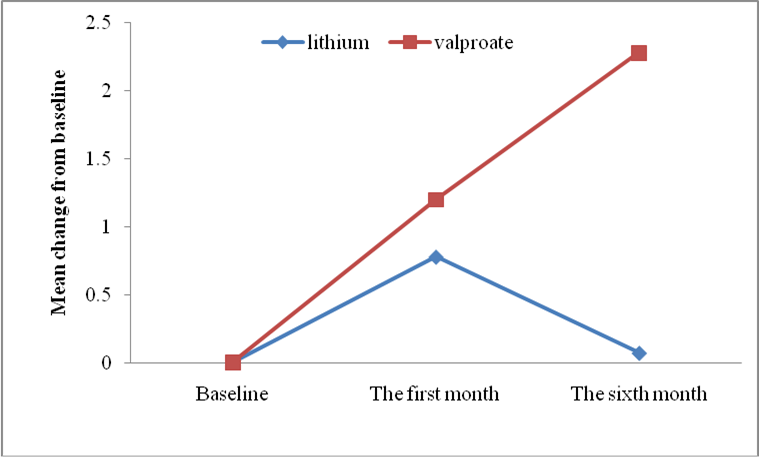
Figure 1: The effects of taking lithium or sodium valproate on the percentage of body fat (PBF) in patients
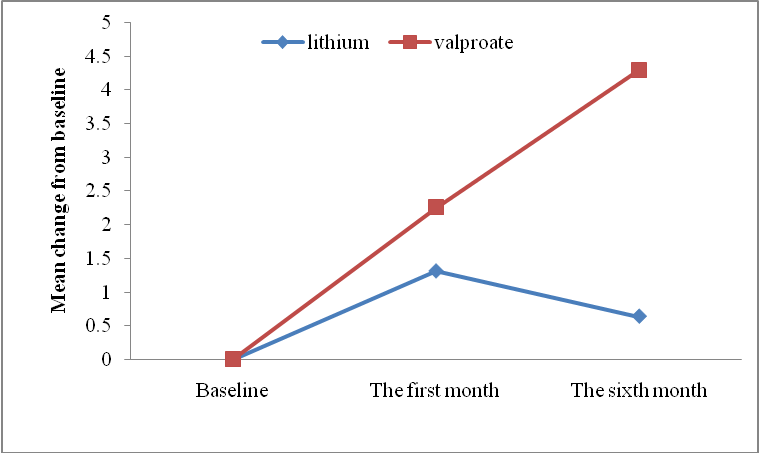
Figure 2: The effects of taking lithium or sodium valproate on weight gain in patients (kg)
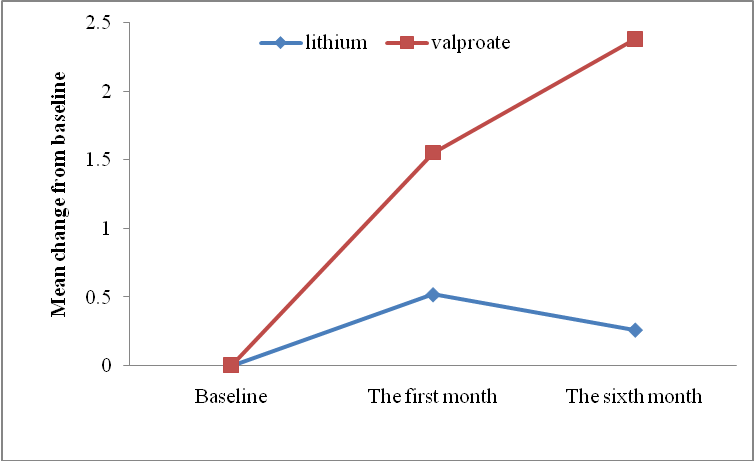
Figure 3: The effects of taking lithium or sodium valproate on body mass index (BMI) in patients (kg/m2)
Discussion
In the present study, we aimed to compare the effects of the initiation of lithium and valproate on body composition indexes in patients with type I bipolar disorder who were referred from an outpatient clinic to our center.
While we observed a significant increase in average body weight among the valproate group, lithium had no considerable effect on the investigated body composition parameters during the six-month duration of the study. We observed a 2.3 kg/m2 increase in BMI in patients treated with valproate, which was similar to previous studies, such as a study that reported a BMI increase of 2-4 kg/m2 by valproate15-18. Sandra et al. showed that the proportion of visceral fat in patients who consumed valproate for 11 years increased by 7%19. Bayram et al. have also supported our findings and observed that treatment with valproate in epilepsy patients was associated with weight gain20. Other studies have demonstrated that either short-term or long-term valproate therapy could lead to an increase in body weight, fat accumulation, and, as a result, a rise in BMI15,21. There is also evidence indicating that valproate is related to an increase in the level of insulin and leptin density in the serum15.
Valproate’s effects on serotonin levels may be the primary underlying cause of weight gain20. In this scenario, it is suggested that valproate decreases the level of serotonin in the central nervous system. Lower levels of serotonin are associated with greater carbohydrate consumption and increased appetite23,24. Impaired sympathetic nervous system, genetic susceptibility, leptin resistance, and hyperinsulinemia due to increased secretion of β-cells are other alternative pathways to justify increases in body weight induced by valproate15,24,25.
While our findings are consistent with some prior studies, there also exist studies with contrasting results. For example, Chengappa et al. reported that lithium and valproate were associated with 8.2% and 8.5% weight gain, respectively (p-value > 0.05), and the increase in BMI was reported at 2.1 kg/m2 for both drugs8. The difference between our results and their results may be due to the difference in sample sizes and study durations (their sample included 214 patients and the duration of follow-up was 12 months). However, while their study was not limited to monotherapy treatment, our study strategically included only monotherapy treatment to reduce confounding variables with the goal of achieving more reliable results. Furthermore, a meta-analysis by McKnight et al. showed that lithium caused 1.89 times more weight gain than the placebo group11.
Lithium has been compared to other mood stabilizing medications as well. Coxhead et al. compared weight gain in patients taking lithium versus carbamazepine and reported that weight increased by 4 kg and 3.1 kg, respectively, over 12 months26. Their study showed a greater weight gain in patients taking lithium compared to our results, which may be attributed to their longer follow-up period26.
In our study, weight gain and change in PBF showed a greater increase within the first month of treatment with lithium, but the increase slowed down within six months. Treatment with valproate, however, showed increases in weight gain and PBF even after six months of treatment. This is an important aspect to be considered by clinicians that observe initial weight gain in the management of their patients.
We did not find a significant increase in TBW percentage in either the lithium or valproate groups during our study. Another significant clinical finding was that the gained weight in patients treated with valproate was not due to excess water retention in extracellular space. Our finding regarding TBW was similar to the study by Bayram et al., who showed no statistically significant increase in TBW among epileptic patients treated with valproate acid20.
Although the mean SLM change was slightly higher in the valproate group, no statistically significant difference was found in either the lithium or valproate groups. In the current study, the mean change in SLM in the valproate group was 1.3 kg over the six-month treatment course, whereas another study reported a 4 kg increase in lean mass accumulation20. The main difference between these two studies was the study population. We performed the study on adults, while Bayram et al. evaluated valproate effects on epileptic children which may have received different dosage too20. It seems that valproate has the potential to increase SLM, but more research is required in this regard.
Limitations
The current study has several limitations that must be considered in the interpretation of our findings. The small sample size was our first limitation. Additionally, we had a limited follow-up duration and followed patients for only six months. These limitations may reduce the generalizability of our findings, and multi-center clinical trials with long-term follow-up are required to evaluate the same hypothesis. A record of daily food intake or a food diary and a record of physical activity levels may help collect more accurate and justified data. However, we optimized the accuracy of our findings by restricting the study to adult patients who had not recently taken either studied medication and were on monotherapy to reduce confounding variables.
Conclusion
In conclusion, among patients with bipolar I disorder, valproate was associated with a greater increase in multiple body composition indexes over six months, including body weight, BMI, and PBF when compared to lithium. Initial weight gain in patients treated with lithium slowed down within six months of treatment, an effect that must be considered in long-term patient care management.
List of abbreviations
Bioelectric impedance analysis (BIA); body mass index (BMI); percentage of body fat (PBF); soft lean mass (SLM); total body water (TBW).
Authors' contributions
The authors confirm contribution to the paper as follows: study conception and design: S.B., S.A., A.S.; data collection: M.P., Z.M., M.M.; analysis and interpretation of results: S.B., S.A., M.M., S.M.; draft manuscript preparation: S.A., A.S., M.M.; All authors reviewed the results and approved the final version of this manuscript.
Acknowledgment
The authors are thankful to the patients and staff at the Department of Psychosomatic Medicine, Taleghani Hospital Research Development Committee, Shahid Beheshti University of Medical Sciences (SBMU) who made this study possible. No funding was provided for this study.
References:
- GBD 2015 Eastern Mediterranean Region Mental Health Collaborators. The burden of mental disorders in the Eastern Mediterranean region, 1990-2015: findings from the global burden of disease 2015 study. Int J Public Health. 2017; 63(Suppl 1): 25-37. doi: 10.1007/s00038-017-1006-1. Epub 2017 Aug 3. PMID: 28776247; PMCID: PMC5973970.
- De Hert M, Cohen D, Bobes J, et al. Physical illness in patients with severe mental disorders. II. Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World Psychiatry. 2011; 10(2): 138-51. doi: 10.1002/j.2051-5545.2011.tb00036.x. PMID: 21633691; PMCID: PMC3104888.
- Sarwer DB, Polonsky HM. The Psychosocial Burden of Obesity. Endocrinology and metabolism clinics of North America. 2016; 45(3): 677–688. https://doi.org/10.1016/j.ecl.2016.04.016.
- Vieta E, Günther O, Locklear J, et al. Effectiveness of psychotropic medications in the maintenance phase of bipolar disorder: A meta-analysis of randomized controlled trials. International Journal of Neuropsychopharmacology. 2011; 14(8):1029–49. Available from: https://www.ncbi.nlm.nih.gov/books/NBK82720/.
- Geddes JR, Miklowitz DJ. Treatment of bipolar disorder. Lancet. 2013; 381(9878): 1672-82. doi: 10.1016/S0140-6736(13)60857-0. PMID: 23663953; PMCID: PMC3876031.
- Collins N, Barnes TRE, Shingleton-Smith A, et al. Standards of lithium monitoring in mental health trusts in the UK. BMC Psychiatry. 2010 Oct 12; 10(1): 80. Available from: http://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-10-80.
- Patil P, Schwartz TL. Fine Tuning the Use of Second Generation Antipsychotics. J Ment Health Clin Psychol. 2018; 2(5): 22-39.
- Chengappa KNR, Chalasani L, Brar JS, et al. Changes in body weight and body mass index among psychiatric patients receiving lithium, valproate, or topiramate: An open-label, nonrandomized chart review. Clinical Therapeutics. 2002; 24(10):1576–84. Available from: https://pubmed.ncbi.nlm.nih.gov/12462287/.
- Khan SS, Ning H, Wilkins JT, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiology. 2018; 3(4): 280–7. Available from: https://jamanetwork.com/.
- Torrent C, Amann B, Sánchez-Moreno J, et al. Weight gain in bipolar disorder: pharmacological treatment as a contributing factor. Acta Psychiatr Scand. 2008;118(1): 4-18. doi: 10.1111/j.1600-0447.2008.01204.x. Epub 2008 May 22. PMID: 18498432.
- McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012; 379(9817): 721-8. doi: 10.1016/S0140-6736(11)61516-X. Epub 2012 Jan 20. PMID: 22265699.
- Gitlin M. Lithium side effects and toxicity: prevalence and management strategies. International Journal of Bipolar Disorders. 2016; 4: 27. https://doi.org/10.1186/s40345-016-0068-y.
- Baptista T, Lacruz A, de Mendoza S, et al. Endocrine effects of lithium carbonate in healthy premenopausal women: Relationship with body weight regulation. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2000; 24(1):1–16.
- Treiser SL, Cascio CS, O’Donohue TL, et al. Lithium increases serotonin release and decreases serotonin receptors in the hippocampus. Science [Internet]. 1981; 213(4515):1532–4. https://pubmed.ncbi.nlm.nih.gov/6269180/.
- Rauchenzauner M, Haberlandt E, Scholl-Bürgi S, et al. Effect of valproic acid treatment on body composition, leptin and the soluble leptin receptor in epileptic children. Epilepsy Research. 2008; 80(2–3): 142–9. https://linkinghub.elsevier.com/retrieve/pii/S092012110800082X.
- Ayyagari M, Chitela S, Kolachana V. Obesity, polycystic ovarian syndrome and thyroid dysfunction in women with epilepsy. Annals of Indian Academy of Neurology. 2012; 15(2): 101. http://www.annalsofian.org/text.asp?2012/15/2/101/94992.
- Sahota P, Prabhakar S, Kharbanda PS, et al. Seizure type, antiepileptic drugs, and reproductive endocrine dysfunction in Indian women with epilepsy: A cross-sectional study. Epilepsia. 2008; 49(12): 2069–77. https://pubmed.ncbi.nlm.nih.gov/18503558/.
- Camilla Haw, Arleen Rowell. Obesity and its complications: a survey of inpatients at a secure psychiatric hospital. The British Journal of Forensic Practice. ISSN: 1463-6646. 2011; 13(4): 270-277.
- Petty SJ, Kantor S, Lawrence KM, et al. Weight and fat distribution in patients taking valproate: A valproate-discordant gender-matched twin and sibling pair study. Epilepsia. 2014; 55(10): 1551–7. https://pubmed.ncbi.nlm.nih.gov/25124647/.
- Bayram E, Bayram MT, YiÅ U, et al. Evaluation of the body composition with bioelectrical impedence analysia in epileptic patients treated with valproic acid. Vol. 23, Neurology Asia. 2018; 23(2): 131-136.
- Sidhu HS, Srinivas R, Sadhotra A. Evaluate the effects of long-term valproic acid treatment on metabolic profiles in newly diagnosed or untreated female epileptic patients: A prospective study. Seizure. 2017; 48: 15–21. https://pubmed.ncbi.nlm.nih.gov/28365440/.
- Rosenthal NE, Genhart MJ, Caballero B, et al. Psychobiological effects of carbohydrate- and protein-rich meals in patients with seasonal affective disorder and normal controls. Biological Psychiatry. 1989; 25(8): 1029–40. https://pubmed.ncbi.nlm.nih.gov/2720016/.
- Wurtman JJ. Carbohydrate craving, mood changes, and obesity. J Clin Psychiatry. 1988; 49 Suppl:37–9.
- Kossak BD, Schmidt-Sommerfeld E, Schoeller DA, et al. Impaired fatty acid oxidation in children on valproic acid and the effect of L-carnitine. Neurology. 1993;43(11): 2362–8. https://pubmed.ncbi.nlm.nih.gov/8232957/.
- Verrotti A, Basciani F, Morresi S, et al. Serum leptin changes in epileptic patients who gain weight after therapy with valproic acid. Neurology. 1999; 53(1): 230–2. https://pubmed.ncbi.nlm.nih.gov/10408570/.
- Coxhead N, Silverstone T, Cookson J. Carbamazepine versus lithium in the prophylaxis of bipolar affective disorder. Acta Psychiatrica Scandinavica. 1992; 85(2), 114-118.