
A Peer-Support Mental Health Response Training for LGBTQIA+ Adolescents
Megan Chernosky*
University in Louisville, Kentucky, USA
Abstract
This paper will discuss the correlation between participation in a mental health peer-support training and adolescents’ self-reported feelings of preparedness to deal with mental health crises. The paper will focus on lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other non-heterosexual, non-cisgender youth (LGBTQIA+) between the ages of 13 and 21 years old. The study used a quantitative, written survey with eighteen questions before the intervention, and another with five questions after the intervention. The study originally involved eleven participants, but the number of participants decreased to seven dues to attrition. The intervention was administered to every participant. The data were analyzed to find the averages and standard deviations for each category. The results found that the average preparedness increased after the intervention. Due to lack of a control group, the researcher was not able to determine causation, but they were able to determine correlation. The researcher concluded that there was a short-term increase in feelings of preparedness to deal with crises in correlation with receiving the mental health training.
Introduction
Mental health crises are a significant problem for adolescents and almost one in two adolescents will struggle with some form of mental illness by the time they turn 18.
Adolescents have less independence than adults do. They do not have the ability to seek help from a professional in the same way adults do without parental consent. As a result, teenagers tend to have less access to mental health care professionals than adults do. The first hypothesis that the researcher wanted to test was that adolescents are more likely to seek help from other adolescents than they are professionals or other adults in authority. The second, related hypothesis is that lesbian, gay, bisexual, transgender, queer, intersex, and asexual (LGBTQIA+) youth are more likely to talk to people their own age instead of mental health professionals if they have not disclosed their identity to their parents.
Assuming the above hypotheses to be true, LGBTQIA+ adolescents need to be trained on how to respond to mental health crises. The researcher analyzed other, similar mental health gatekeeper trainings in order to design a training that would work for adolescents. The training was intended to teach adolescents how to respond if a peer were to come to them during a mental health crisis. It was very clear that it was not intended to train the youth as a mental health counselor or therapist. The training was intended to teach them to deal with the emergency if there is one and then connect the individuals with resources that could help them.
The third and primary hypothesis of the researcher was that the described training would increase adolescents’ self-reported feelings of preparedness to deal with mental health crises. The researcher focused on the most common mental health crises in order to maximize the utility of the training.
The Center for Behavioral Health Statistics and Quality performs an annual report to determine the lifetime prevalence of mental illness for adolescents under the age of 18. That term means the percentage of adolescents who have experienced a given mental illness before they turn eighteen. The 2016 report stated that 46.30% of adolescents will experience some form of mental illness before they turn 18. The three most common types of disorders are anxiety disorders, mood disorders, and major depressive disorder, with lifetime prevalence of 25.10%, 14.00%, and 11.20%, respectively. One of the biggest risks for people with mental illness is suicide. Suicide is the second leading cause of death for adolescents between the ages of 15 and 24. It is estimated that in 2015, the rate of suicide for adolescents was 12.5 out of every 100,000, but the rate increased to 13.7 out of every 100,000 in 20161,11. Suicide rates have been consistently increasing since 20081,4.
Additionally, while no agency collects data on the rate of adolescents who attempt suicide, the American Foundation for Suicide Prevention predicts that 25 people attempt suicide for everyone person who completes, indicating that 342.5 adolescents out of every 100,000 attempt suicide each year1. The United States Census Bureau estimates that there are 41,731,233 people between the ages of 10 and 19 in the United States in 2015, meaning that approximately 142,930 adolescents attempt suicide each year18. Other estimates put that number far higher, at two million4.
According to the Center for Disease Control, lesbian, gay, and bisexual adolescents are five times more likely to complete suicide as compared to their heterosexual counterparts (2016). The Williams Institute estimates that 45% of transgender individuals will attempt suicide by the time they turn 247. This risk increases significantly when an LGBTQIA+ adolescent is not accepted by their family6. An adolescent with an unaccepting family is eight times more likely to attempt suicide as compared to their peers with accepting 93 families4.
Adolescents are at a stage in their lives where they are less likely to trust in adults than they did when they were younger20. This is generally a natural part of development. It increases independence, which is a skill that helps an individual in young adulthood20. However, due to the lack of trust in adults, and the relative inexperience of adolescents as compared to adults, when an adolescent experiences a crisis, they often do not have the resources to deal with crises on their own14. They will often turn to their peers for help instead of adults8,10. As a result, training adolescents may prove another strategy for dealing with adolescent crises8.
LGBTQIA+ adolescents are less likely to have accepting families as compared to cisgender heterosexual adolescents16. They are particularly more likely to have stronger relationships with their peers than their families, and thereby more likely to seek support from their peers13. It is also shown that LGBTQIA+ adolescents are disproportionately more likely to seek support from other LGBTQIA+ adolescents21. This is especially true in isolating situations22.
Intervention Literature Review
The researcher analyzed several similar studies to maximize success of the training.
In a quantitative, non-experimental study performed by Mitchell, Kader, Darrow, Haggerty, and Keating, researchers wanted to test if an intervention called Question, Persuade, Refer (QPR) would increase college students’ knowledge of the warning signs of suicide, knowledge of how to ask someone about suicide, and knowledge of how to get help for someone who was experiencing thoughts of suicide11. The original sample size was 1,644 college students, but only 274 completed all of the steps of the study. The college students’ knowledge of the warning signs of suicide, knowledge of how to ask someone about suicide, and knowledge of how to get help for someone who was experiencing thoughts of suicide was measured through a survey of eleven questions. In ten of the questions, participants were asked to rate their level of knowledge and level of comfort, on a scale of one to three. One was a yes-or-no question, where participants were asked about their previous experiences with referring someone to help for suicidal ideation or actions. The researchers did mention in their study that the survey is not empirically validated, but it is a survey that comes with the QPR training. The subjects’ knowledge was measured at three points in the process. The first was before the intervention, then again post intervention, and then again in a three month and a six-month follow-up. The researchers found that “knowledge of the warning signs of suicide, how to ask someone about suicide, persuading someone to get help, how to get help for someone, and local resources to help with suicide increased significantly in the short-term, and these gains were maintained over the long-term”11. However, participants’ level of comfort in asking someone about whether or not they would commit suicide, which is an important part of the QPR intervention, increased initially, but returned to their baseline during the follow-up assessment11. There was overall a high correlation between those who undertook the study and those who felt more comfortable intervening in crises.
Jacobson, Osteen, Sharpe, and Pastoor performed a mixed method experiment in 20129. They sought to test if a QPR training would improve “knowledge of suicide warning signs and intervention behaviors, self evaluation of suicide prevention knowledge, and knowledge of institutional resources” among University of Maryland Baltimore Campus Masters of Social Work (MSW) students9. One hundred nineteen students were randomly selected from the Masters of Social Work program, and 72 students completed the study. They randomly assigned the subjects into either the intervention group or the control group, which did not receive any intervention or training. The experiment resulted in the researchers concluding that people’s attitudes about suicide, specifically, asking people whether or not they were going to commit suicide, did not change as a result of the experiment, but the participants did tend to perceive that they were better prepared to handle those situations and had better knowledge of institutional resources as a result of the intervention.
Hadlaczky, Hokby, Mkrtchian, Carli, and Wassmerman constructed a meta-analysis of the literature surrounding Mental Health First Aid6. They summarized the results of fifteen papers dedicated to reviewing Mental Health First Aid. It particularly focused on three areas of review. The first was the effect of the Mental Health First Aid training on the subjects’ knowledge surrounding mental health issues. The second was the effect of the Mental Health First Aid training on the subjects’ attitudes towards people with mental health issues. The third effect studied was effect of the Mental Health First Aid training on the subjects’ behavior towards individuals with mental health problems. Each of the fifteen studies used a quantitative survey of the participants after the training in order to determine the change in knowledge, attitude, and behavior. The meta-analysis concluded that the Mental Health First Aid training increased overall knowledge of mental health problems, including symptomatology and treatment, decreased negative attitudes towards people with mental health issues, and increased supportive behavior towards individuals with mental illness.
A similar intervention to the QPR training and the Mental Health First Aid training is the Peer2Peer training19. A Peer2Peer training was completed by Vadja at the Medical University of Graz in 2016. The Peer2Peer study is slightly more complicated than the QPR or Mental Health First Aid studies, because it tracked the number of contacts that were made by the people who were trained. It was intended to track specifically whether or not the training resulted in interventions. The initial study trained 119 subjects in responding to mental health crises. Training those 119 subjects resulted in a total of 94 interventions during the monitoring period. The researchers described the study as a success, due to the increase they observed in “practical skills in dealing with students in crises situations”19.
Peer Gatekeeper Training (PGT) was another of these types of trainings that was tested at eight schools in the southern part of Vancouver Island in Canada17. To control the variables, the researchers sampled strategically in a way that included representation from each of the school districts in the area, and a secular private school, and a religious school. The sample measured 65 adolescents, including individuals between the ages of 13 and 18, with an average age of 15.6. The training was designed to measure skills in intervening and attitudes towards mental illness. Stuart, Waalen, and Haelstromm, the researchers who conducted the experiment, determined that “significant differences in skills, attitudes toward suicide intervention, and knowledge occurred after training and were maintained in all areas over a 3-month period of time”17.
Several of the studies had overlapping aspects. One of the more significant aspects was an acronym, which has been proven to increase memory2. QPR uses the acronym QPR, and Mental Health First Aid uses the acronym ALGEE. All studies above also discussed a mental health peer gatekeeper training, and found that it positively correlated with an increase in the subjects’ ability to respond to mental health crises. There was some discrepancies between whether or not these trainings were correlated with long-term change.
Materials and Methods
Once the training was designed, it was approved by the human subjects board at University of Louisville on January 25, 2018. The human subjects board approved an assent for the participants under eighteen, because the risk of informing parents that their child was to participate in a study on LGBTQIA+ adolescents was believed to be riskier than the study itself. The study was conducted through a local agency in Louisville, Kentucky, which shall remain unnamed in order to protect the confidentiality of the participants in the study. The agency has access to numerous adolescents who identify as LGBTQIA+ and their allies. The researcher volunteers at the agency and coordinated with the leaders of the agency in order to conduct the study there. The study was conducted on January 26, 2018. Approximately thirty adolescents came to the agency on that night, and were told the nature of the survey. Nineteen adolescents elected not to participate in the study, and eleven participated.
The intervention began with the consent or assent documents, and then each participant took the initial assessment. The assessment included a demographic assessment, covering age, race/ethnicity, gender identity, and sexual orientation. The assessment also asked to whom the participant had disclosed their sexual orientation and gender identity, what experiences they had with mental health crises, what resources they had if they had a mental health crisis, and their level of preparedness to deal with mental health crises. Preparedness was assessed on a five-point scale from very prepared to not at all prepared, asking about panic attacks, anxiety attacks, depression and hopelessness, suicidal thoughts, and suicidal actions.
The training was provided in a slide presentation. The presentation was primarily administered by the researcher, but there were some interactive activities as well. The first topic brought up in the slide presentation was a trigger warning in order to minimize traumatization. The researcher knew that several of the participants could potentially be triggered by suicide, and wanted to ensure that they were not triggered. The training focused the CLOG acronym, which stands for Check for risk of harm, Listen non-judgmentally, Offer encouragement, and Give resources for professional support. An acronym was used in order to improve recollection2. Then the intervention discussed how the acronym could be used for each type of mental health crisis, starting with suicide, and proceeding on to discuss depression, self-injury, and panic attacks. It concluded by discussing self-care for the participants. The second survey was given immediately after the investigation. It was considerably shorter, including only the five-point scale on how prepared they feel to deal with specific types of mental health crises.
A trifold brochure with six panels was provided to the participants after the presentation to reinforce the training. The inside panel of the brochure, the one that is the first to be seen upon opening the brochure, includes the acronym CLOG, along with what each letter stands for and some tips for orchestrating each of the steps. Once the brochure is open, the two panels on either side feature tips for dealing with suicide, panic attacks, depression, and self-harm. It also gives layperson definitions. The center panel also features an easy-to-follow risk assessment diagram proven to be effective for laypeople to use15. The back of the brochure discussed several resources that they could use, including several hotlines and resources in the area. The brochures are available at the agency for anyone to take if they need it.
Results
The total number (N) of people who took the initial survey was eleven, and 7 people completed the intervention. The average age of participants was 15.95. Ten of the participants identified as white or caucasian. One identified as Native American and mixed. Five participants identified as women, five identified as non-binary, and one identified as a man. Seven identified as transgender, and four identified as cisgender. None of the participants identified as heterosexual. Seven of the participants said that they had disclosed their identity as LGBTQIA+ to their parents, and three said that they had not disclosed their identity. One response was unclear.
Every participant said that they had a friend who had a problem with mental health. Ten of them said they had a friend come to them with a mental health crisis. The most common was suicide ideation, followed by anxiety and depressive episodes, followed by panic attacks.
Ten of the eleven participants said they had a trusted adult in their life. Seven of the eleven participants said they talked to a mental health professional. Ten of the eleven participants said they had a trusted peer in their life. Of the eleven participants, seven said they could reach an adult in case of a crisis, and ten said they could reach a peer in case of a crisis. In case of crisis, six participants said they would go to a peer, five said they would talk to an adult, three said they would talk to a mental health professional, and one said they would talk to an anonymous hotline.
Identity disclosure
One-third of the individuals who had not disclosed their LGBTQIA+ identity to their parents said that they did not have an adult they could trust. All of the individuals who had disclosed their identity to their parents said that they had an adult they could trust. Two out of the three people who said they had not come out to their parents said that they could not reach a trusted adult if they had a crisis, while one out of seven individuals who said that they had come out to their parents said that they could not reach a trusted adult if they had a crisis. Two out of the three individuals that said they had not come out to their parents said that they would go to a peer if they had a mental health crisis as opposed to a trusted adult, compared to two out of seven individuals who had come out their parents who said that they would go to a peer if they had a mental health crisis as opposed to a trusted adult.
Preparedness to deal with crises
The next series of questions on the assessment given before the intervention asked how prepared the participant felt to deal with a mental health crisis if a peer came to them about it. It was identical to the assessment given after the training. It asked them to rate how prepared they felt on a Likert scale of one to five, with five being very prepared and one being not prepared at all. Every participant answered every question.
The average level of preparedness for dealing with all mental health crises before the intervention was approximately 3.29. The average level of preparedness for dealing with all mental health crises after the intervention was approximately 4.11. The t-test results in a value of approximately 1.79. Using the alpha value of 0.05, these results are statistically significant. Those statistics were found by analyzing all responses to all questions. The data in this section is presented in Figure 1.
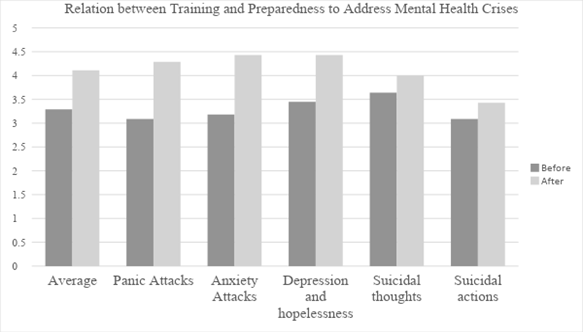
Figure 1: Mean Response to Preparedness Survey, Before and After
Panic attacks: The first question addressed how prepared the participant felt to deal with someone having a panic attack. The average that was determined for the assessment before the intervention was approximately 3.09. The average determined for the assessment given after the intervention was approximately 4.29. This was an increase in average preparedness of approximately 1.2. The t-test results in a value of approximately 1.86. Using the alpha value of 0.05, these results are statistically significant.
Anxiety attacks: The second question asked how prepared the participant felt to deal with someone having an anxiety attack. The average determined for the assessment before the intervention was approximately 3.18. The average determined for after the intervention was approximately 4.43. This resulted in an increase in average preparedness of approximately approximately 1.25. The t-test results in a value of approximately 1.94. Using the alpha value of 0.05, these results are statistically significant.
Depression and hopelessness: The third question asked how prepared the participant felt to help someone experiencing depression and hopelessness. The average calculated for the assessment before the intervention was approximately 3.45. The average calculated for the assessment after the intervention was approximately 4.43. This resulted in an increase in average preparedness of approximately 0.98. The t-test results in a value of approximately 1.7. Using the alpha value of 0.05, the results are not statistically significant.
Suicidal thoughts: The fourth question addressed how prepared the participant felt to deal with someone experiencing suicidal thoughts. The average determined for the assessment given before the intervention was approximately 3.64. The average determined for the assessment given after the intervention was approximately 4.00. This means that there was an increase in the average preparedness of approximately 0.36. The t-test results in a value of approximately 1.97. Using the alpha value of 0.05, the results are statistically significant.
Suicidal actions: The fifth question asked how prepared the participant felt to deal with someone who has taken action to attempt suicide. The average calculated for the data taken before the intervention was approximately 3.09. The average calculated for the data taken after the intervention was approximately 3.43. This means that there was an increase in average preparedness of 0.34. The t-test results in a value of approximately 1.72. Using the alpha value of 0.05, the results are not statistically significant.
Discussion
The researcher was able to conclude that, in the population of LGBTQIA+ adolescents who participated in the study, there was a correlation between the mental health intervention training and an increase in self-reported feelings of preparedness to deal with mental health crises. That correlation was statistically significant in the fields of panic attacks, anxiety attacks, and suicidal thoughts. This supports the third and primary hypothesis of the researcher.
Every category of the mental health crisis that was assessed demonstrated an increase in self-reported preparedness. The self-reported feelings of preparedness increased the most for dealing with anxiety attacks, and increased the least for preparedness to deal with suicidal actions. Before the intervention, individuals felt the most prepared to deal with suicidal thoughts, and least prepared to deal with suicidal actions and panic attacks. After the intervention, individuals felt most prepared to deal with depression and hopelessness and anxiety attacks, and least prepared to deal with suicidal actions.
The first hypothesis that adolescents were more likely to turn to a peer for help during a crisis as compared to an adult, was partially supported, although it was not as strongly supported as anticipated. The researcher found that six people said that they would go to a peer for support, as opposed to five people that said that they would go to a trusted adult that was not a mental health professional, and three said they would talk to a mental health professional. More people said they would go to a peer as opposed to any other category, but more people said they would go to some type of adult rather than a peer.
When looking specifically at adolescents who had not disclosed their LGBTQIA+ identity to their parents, these adolescents were less likely to have an adult that they could trust in their life. Therefore, they were less likely to turn to a trusted adult, as compared to their peers. This research supported the second hypothesis, that LGBTQIA+ youth are more likely to talk to people their own age if they have not disclosed their identity to their parents.
Limitations of the Research
Due to the sample size, it is not possible to randomize the data, assess causation, or assess outlying pieces of data, which increases the likelihood of incorrect data. The sample also was not obtained randomly, as it was obtained simply through clients at an agency. As such, the data is merely representative of the seven adolescents who completed the intervention, not of the population as a whole.
Conclusion
Many adolescents find it challenging to obtain mental health care through a trained professional, especially during a time of crisis. It may be helpful to redo this training with a larger sample size and with the ability to have a control group in order to determine if the conclusions from this study are accurate and are generalizable to a larger population. Having more resources may also allow testing for the long-term recall effects, as some of the studies mentioned in this paper were able to do. It may be advantageous to control for the location, by doing similar studies in other cities, particular cities in other cultures. In these areas, research should be conducted in a way that finds samples representative of the larger population as a whole, including LGBTQIA+ adolescents who are from varying socioeconomic statuses and varying races or ethnicities, as the sample in this study did not include a variety of racial backgrounds. If such a study is conducted, it may be advantageous to define the sexual orientations and gender identities listed in the survey. While the group of participants above knew what all of the terms meant, it is possible that a group that was not as homogenous as the participants may not. It may also be advantageous to compare LGBTQIA+ adolescents to heterosexual, cisgender adolescents, or to compare LGBTQIA+ adolescents whose parents have negative reactions with LGBTQIA+ adolescents whose parents have positive reactions.
It may be wise to test this with other populations that are difficult to reach for mental health care, like the population of people experiencing homelessness or a population of people dealing with substance abuse. This strategy should theoretically make it easier for any marginalized population without access to traditional mental health care to learn to deal with mental health crises.
Additionally, the researcher is also interested in determining if adolescents, especially LGBTQIA+ adolescents, are more likely to confide in their peers as compared to adults. This research could be done through a survey of adolescents, particularly LGBTQIA+ adolescents. The training would not need to be administered to assess to whom adolescents would go to in case of a crisis. The idea of doing a nationwide survey of LGBTQIA+ adolescents is not unfeasible. Every other year, the Gay Lesbian-Straight Education Network completes a survey of LGBTQIA+ adolescents in schools to determine their educational experience9. If a larger survey of the population confirms the findings of this study, it would be interesting to assess why LGBTQIA+ adolescents who have not disclosed their identity tend to trust their peers more than adults.
Based solely on the findings of this study, which is not generalizable to the population as a whole, it may be more advantageous for practitioners to find a handful of members of a marginalized or isolated population and train them to respond to mental health crises. This training may help other individuals, if the trained individual is able to help them. While this is not a permanent solution to the problem of the high rates of mental illness and suicide, as it does not provide a trained professional using research-informed interventions, it does at least provide a temporary solution that may keep someone alive for long enough to be able to seek that mental health care that they need.
Acknowledgements
The author would like to thank her thesis defense committee, Dr. Sunshine Rote, Dr. Janet Woodruff-Borden, and the chair of the committee, Dr. Maurice Gattis, for their work in developing the thesis paper.
References
- American Foundation for Suicide Prevention. Suicide Statistics. 2018. Retrieved from: https://afsp.org/about-suicide/suicide-statistics/.
- Campos A, Camino E, Pérez-Fabello MJ. Using the keyword mnemonics method among adult learners. Educational Gerontology. 2011; 37(4): 327-335. doi: 10.1080/03601271003608886.
- Center for Disease Control. Sexual Identity, Sex of Sexual Contacts, and Health-Risk Behaviors Among Students in Grades 9-12: Youth Risk Behavior Surveillance. Atlanta, GA: U.S. Department of Health and Human Services. 2016.
- Dilillo D, Mauri S, Mantegazza C, et al. Suicide in pediatrics: epidemiology, risk factors, warning signs and the role of the pediatrician in detecting them. Italian journal of pediatrics. 2015; 41(1): 49. https://doi.org/10.1186/s13052-015-0153-3.
- Haas AP, Eliason M, Mays VM, et al. Suicide and Suicide Risk in Lesbian, Gay, Bisexual, and Transgender Populations: Review and Recommendations. Journal Of Homosexuality. 2011; 58(1): 10-51. doi:10.1080/00918369.2011.534038.
- Hadlaczky G, Hökby S, Mkrtchian A. Mental Health First Aid is an effective public health intervention for improving knowledge, attitudes, and behaviour: A meta analysis. International Review of Psychiatry. 2014; 4: 467-475. doi: 10.3109/09540261.2014.924910.
- Herman J, Haas A, Rodgers P. Suicide attempts among transgender and gender nonconforming adults. Los Angeles: The Williams Institute, UCLA. 2014.
- Kalafat J, Elias M. An evaluation of a school?based suicide awareness intervention. Suicide 361 and Life-Threatening Behavior. 1994; 24(3): 224-233. doi: 10.1111/j.1943-278X.1994.tb00747.x.
- Jacobson JM, Osteen PJ, Sharpe TL, et al. Randomized Trial of Suicide Gatekeeper Training for Social Work Students. Research On Social Work Practice. 2012; 22(3): 270-281. doi:10.1177/1049731511436015.
- Kosciw J, Greytak E, Giga N, et al. The 2015 National School Climate Survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation’s schools. New York: GLSEN. 2016.
- Mitchell SL, Kader M, Darrow SA, et al. Evaluating Question, Persuade, Refer (QPR) Suicide Prevention Training in a College Setting. Journal Of College Student Psychotherapy. 2013; 27(2): 138-148. doi:10.1080/87568225.2013.766109.
- Murphy SL, Xu JQ, Kochanek KD, et al. Deaths: Final data for 2015. National Vital Statistics Reports; vol 66 no 6. Hyattsville, MD: National Center for Health Statistics. 2017.
- Mustanski B, Newcomb ME, Garofalo R. Mental Health of Lesbian, Gay, and Bisexual Youths: A Developmental Resiliency Perspective. Journal Of Gay & Lesbian Social Services. 2011; 23(2): 204-225. doi:10.1080/10538720.2011.561474.
- Roe SL. Examining the Role of Peer Relationships in the Lives of Gay and Bisexual Adolescents. Children & Schools. 2015; 37(2): 117-124. doi:10.1093/cs/cdv001.
- Runeson B, Odeberg J, Pettersson A, et al. Instruments for the assessment of suicide risk: A systematic review evaluating the certainty of the evidence. Plos ONE. 2017; 12(7). 1-13. doi:10.1/journal.pone.0180292.
- Ryan C, Russell ST, Huebner D, et al. Family acceptance in adolescence and the health of LGBT young adults. Journal of Child and Adolescent Psychiatric Nursing. 2010; 23(4): 205- 213.
- Stuart C, Waalen PhD JK, Haelstromm E. Many helping hearts: An evaluation of peer gatekeeper training in suicide risk assessment. Death Studies. 2003; 27(4): 321. doi: 386 10.1080/0748118039099082.
- US Census Bureau. (2016, June). Annual Estimates of the Resident Population for Selected Age Groups by Sex for the United States, States, Counties, and Puerto Rico Commonwealth and Municipios: April 1 2010 to July 1 2015.
- Vajda C. "Peer2Peer" – A university program for knowledge transfer and consultation in dealing with psychosocial crises in med-school and medical career. GMS Journal For Medical Education. 2016; 33(4): 1-11. doi:10.3205/zma001051.
- Venta A, Shmueli-Goetz Y, Sharp C. Assessing attachment in adolescence: A psychometric study of the Child Attachment Interview. Psychological Assessment. 2014; 26(1): 238. doi:1037/a0034712 396 20.
- Wilkerson JM, Schick VR, Romijnders KA, et al. Social Support, Depression, Self-Esteem, and Coping Among LGBTQ Adolescents Participating in Hatch Youth. Health Promotion Practice. 2017; 18(3): 358-365. doi:10.1177/152483991665446121.
- Willging CE, Israel T, Ley D, et al. Coaching mental health peer advocates for rural LGBTQ people. Journal Of Gay & Lesbian Mental Health. 2016; 20(3): 214-236. doi:10.1080/19359705.2016.1166469.