
A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers
Simon Xin Min Dong
International Institute of Consciousness Science®, Vancouver, BC, Canada
Abstract
The first detailed description of the morphology of gastric ulcer was reported ~230 years ago, but the mechanism has yet to be elucidated. Moreover, peptic ulcers, including duodenal and gastric ulcers, are currently considered an infectious disease caused by Helicobacter pylori, but how the infection leads to ulceration remains elusive. To address these challenges, a recently published Complex Causal Relationship was applied to analyze the existing data. Peptic ulcers were identified as a psychosomatic disease triggered by psychological stress, where Helicobacter pylori plays a secondary role in only the late phase of the disease. This etiology explained all the characteristics and observations/phenomena of peptic ulcers in a series of 6 articles. This second article focused on the pathogenesis of gastric ulcers. Based on hereditary predisposition, the accumulation of past life experiences incurs the formation of a negative lifeview. Consequently, the individual tends to negatively evaluate themselves or current life events, leading to acute psychological stress. The psychological stress triggers the release of aberrant neurotransmitters in the central nervous system, which in turn cause the transmission of pathogenic nerve impulses to the stomach, resulting in a ‘pre-ulcer lesion’ in the gastric wall and eventually, gastric ulcer. This psychopathological model elucidated 12 characteristics and 24 observations/phenomena of gastric ulcer, along with the roles of gastric acid, Helicobacter pylori, and NSAIDs. The effectiveness suggests that theoretical research and empirical study are equally important in medical explorations, and the guiding roles of philosophy are indispensable for the major progress of life science and medicine.
Introduction
The first detailed descriptions of the morphology of gastric ulcers was published by Matthew Baillie in 17931, but the mechanism has remained an unresolved mystery for 230 years. Although 13 theories have been proposed to explain the pathogenesis of peptic ulcers (including duodenal and gastric ulcers)2, the predilection sites, the relapse and multiplicity, the bleeding and perforations of gastric ulcers, as well as many other clinical observations/phenomena, have yet to be fully understood3. Unlike duodenal ulcer, which is a gastric acid-related disorder, gastric ulcer can be hypo-, normo-, or hyper-secretion of gastric acid. Thus, Dragutin Schwartz’s dogma, No Acid, No Ulcer, does not fit gastric ulcers, and the underlying mechanism has never been clarified. The decreased acid-peptic activity suggests impaired mucosal defence4,5, which also remains elusive. In addition, the Non-steroidal Anti-inflammatory Drugs (NSAIDs) usage is also believed to be a cause of gastric ulcers, but its role in the disease remains unknown6,7.
In 1987, Marshall proposed that peptic ulcers are an infectious disease cause by the infection of Helicobacter pylori (H. Pylori)8. This etiological theory has been termed Theory of H. pylori2. Currently, gastric ulcer is believed to be strongly associated with H. pylori infection9,10, but its association with the bacterium is less clear than duodenal ulcer5, and how the infection leads to ulceration remains unknown. Since H. pylori is omnipresent, all regions of the stomach should ulcerate equally. However, gastric ulcer is a sharply circumscribed loss of tissue located primarily in the gastric antrum and lesser curvature11, and has a characteristic ‘punch out’ appearance with clean edges, as if it were cut by a knife12,13. Thus, Theory of H. Pylori cannot explain both the morphology and predilection sites of gastric ulcers, along with many other characteristics and observations/ phenomena. Similar to all the other 12 etiological theories in history, Theory of H. pylori cannot identify the roles of gastric acid and NSAIDs in the disease6,7, and cannot explain ‘despite a high prevalence of H. pylori infection in the population, the incidence of gastric ulcers is low’14,15. Interestingly, 50% of gastric ulcer patients may have no H. pylori infection16,17, and many peptic ulcers were found to be unrelated to the bacterium, but to other unidentified factors17,18. Furthermore, how to find a correlation between the infection and psychological stress caused by life events, and why gastric ulcer is a ‘brain-driven event’ with abnormal neurotransmitters in the Central Nervous System (CNS)19, are also massive challenges for Theory of H. pylori. In addition, the similarities and differences between duodenal and gastric ulcers have never been clarified in Theory of H. pylori.
Evidently, all the 13 etiological theories in history, including the most recent Theory of H. pylori, are facing difficulties while explaining the pathogenesis of gastric ulcers. To address these challenges, a recently published Complex Causal Relationship (CCR) with its accompanying methodologies, epistemologies, and way of thinking20 was applied to analyze the existing data, resulting in the birth of a new theory, Theory of Nodes. This new theory addressed all the characteristics, observations/phenomena, controversies, and mysteries of peptic ulcers in a series of 6 articles (Supplementary Table S1). The first article of the series identified the etiology of peptic ulcers and explicitly explained 7 characteristics and 42 observations/phenomena of duodenal ulcers21. This article is the second one, focusing exclusively on the pathogenesis of gastric ulcers. Notably, numerous studies accumulated in history, especially those from 1900 to 1990, were invaluable to elucidate the pathogenesis of gastric ulcers.
Methods
Based on the etiology identified in the first article of the series21, four steps were taken to elucidate the pathogenesis of gastric ulcers. First, a complete pathological process of gastric ulceration was illustrated, during which theoretical deduction was employed and a new psychopathological model was formulated to elucidate the morphology of gastric ulcers. Second, the new model was applied to explain the major characteristics and clinical observations/phenomena of the disease. Third, the roles of gastric acid, H. pylori, and NSAIDs in gastric ulcers were identified. Lastly, the major similarities and differences between duodenal and gastric ulcers were curated in a table.
Results
The complete pathological process of gastric ulcerations
Peptic ulcers were identified as a psychosomatic disease triggered by psychological stress in the first article of the series21. Starting from this etiology, Theory of Nodes divides the entire pathological process of gastric ulceration into early, intermediate, and late phases. Notably, the morphology of gastric ulcer is the key characteristic to understanding many other characteristics of the disease, as well as the roles of gastric acid, H. pylori, and NSAIDs. In addition, each of the three phases described herein is supported by a large amount of existing data.
Early phase: the formation of a negative lifeview
As described previously, what psychosomatic factors induced in the early phase of duodenal ulcer is concrete/tangible hyperplasia and hypertrophy of gastrin and parietal cells in the stomach21. In contrast, what psychosomatic factors induced in the early phase of gastric ulcer is an abstract/intangible attitude, which is also termed lifeview or worldview22, suggesting that the early phase of gastric ulcer is a more subtle psychological process without obvious pathological changes in the human body. The results of a survey conducted with 109 families found that the relatives of gastric ulcer patients had an increased chance of gastric ulcers; whereas the relatives of duodenal ulcer patients tended to suffer from duodenal ulcers12,23, suggesting that heredity plays an important role in developing peptic ulcers. In Theory of Nodes, hereditary predisposition and environmental factors determine that a portion of individuals in the population tends to develop a negative lifeview towards their own status, people, society, particular life events/issues, or some objects in the surrounding environments24,25. A multidimensional case-controlled study discovered that facing similar number of stressful life events, ulcer patients perceived life events more negatively, and had significantly more personality disturbances than the controls26.
In Theory of Nodes, all the life events experienced before, especially the social relationships such as family, community, culture, and spirituality27, were engaged in the formation of an individual’s lifeview via superposition mechanism (Figure 1). 1. Family environments in early life play a baseline role in the development of lifeview, and the mental status of parents significantly influences the mental health of the child28,29 (Figure 1a). 2. The context of schools has deep effects on the mental health of children and youths30 (Figure 1b). 3. Work circumstances, such as what the individual learns from colleagues, friends, and the working environment31, have a strong impact on her/his lifeview and directly influence the individual’s quality of life (Figure 1c). 4. All what the individual sees, hears, or learns from TV, radio, newspapers, or books, will be integrated into her/his lifeview and may affect her/his opinion of specific life events32 (Figure 1d). 5. As her/his life course moves forward, the individual observes people around herself/himself and reflects upon herself/himself, causing changes in beliefs and behaviors33 (Figure 1e). 6. Many other factors or information from the environments, such as religion, also significantly influence the individual’s viewpoint of herself/himself and life events34 (Figure 1f). All what the individual experienced and observed is superposed to form a personalized lifeview, which influences the individual’s reactions to her/his own status quo, or current life events. Positive life events or environmental factors facilitate the formation of a positive lifeview, whereas negative life experiences or environmental factors may result in a negative lifeview31,35,36.
Therefore, anything experienced before, trivial or significant, shapes more or less the individual’s lifeview, indicating the impacts of past life events will not disappear after the life events are over, but are stored in the individual’s memory and continues to impact the individual in the form of ‘lifeview’. Starting from the lifeview, the individual evaluates herself/himself, people, issues, objects, or events in the surroundings. The evaluation can be positive, negative, or uncertain37. Thus, similar to duodenal ulcers, the early phase of gastric ulcers is the superposition of past life experiences, which determine the individual’s psychological response to current life events. Notably, a negative evaluation is usually not for everything, but for those closely related to the individual.
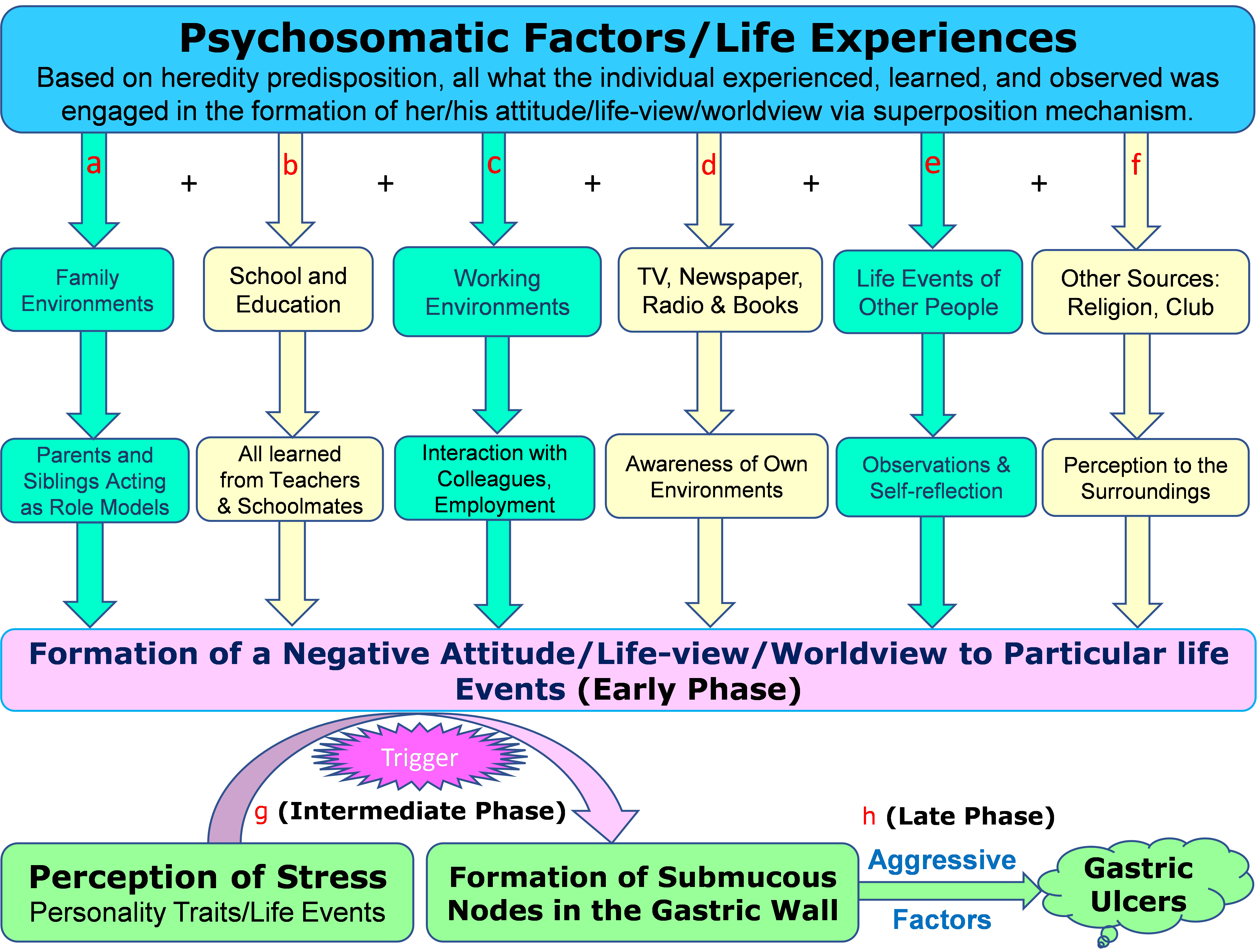
Figure 1: The formation of a negative lifeview based on superposition mechanism.
Heredity predisposes the individual to develop a negative lifeview that is associated with past life experiences. (a) Family environments play a baseline role in the development of lifeview, and parents and siblings are role models of the individual. (b) Schools and education play a central role in the formation of lifeview; teachers and schoolmates significantly influence the mental health of an individual. (c) Colleagues, friends, and working environment add value to the individual’s lifeview. (d) Information from TV programs, radio, newspapers, or books significantly influences the lifeview of an individual and may determine her/his opinion of specific life events. (e) What the individual witnessed of others shapes her/his lifeview. (f) Many other factors from the outside world, such as religion, significantly impact the development of lifeview. (g) In the intermediate phase, the negative life-view potentiates life event/personality trait-induced psychological stress, resulting in the formation of submucous nodes in the gastric wall. (h) The late phase is a corrosive process caused by the local aggressive factors in the stomach, such as gastric acid and H. pylori.
Intermediate phase: stress-triggered formation of submucous nodes
An individual with a negative life-review tends to pessimistically assess her/his own status or negatively respond to specific current life events, causing psychological stress. As described earlier21, the psychological stress leading to duodenal ulcers is usually long-term and chronic, such as bad habits, poor life style, laborious work, unhealthy environment, and/or long-term emotional distress38, whereas the psychological stress causing gastric ulcers is usually short-term and acute, such as crucial social or family events, natural disasters, or sudden loss of a family member. This kind of acute stress can be simulated easily in labs39,40 and therefore, stress-induced ulcers in labs are usually gastric ulcers19. Similar to duodenal ulcers, the intermediate phase of gastric ulcer is also a short-term process, but characterized by stress-triggered pathological lesions in the gastric wall (Figure 1g). Many psychosocial factors, such as personality traits, family or social events, seasonal changes, working environments, or natural disasters may cause acute psychological stress, which eventually triggers gastric ulceration16,41–43. As illustrated previously, the sources of psychological stress are not limited to life events21, but may be spontaneous without the experience of any life event, such as personal threat and goal frustration44.
Similar to duodenal ulcers, the consequence of psychological stress in gastric ulcers is the abnormal release of neurotransmitters in the CNS, causing the transmission of pathogenic nerve impulses to the stomach. Numerous studies demonstrated that gastric ulcer is a ‘brain-driven event’ with abnormal neurotransmitters in the CNS, and the amygdala and hippocampal formation are the brain sites for modulating stress-induced gastric erosions19. Stimulation or lesions of the central nucleus of the amygdala produced or reduced gastric ulcers, respectively45. Further, cold stress-induced ulcers in mouse models could be controlled by intraperitoneal pre-treatment with Ethylenediaminetetraacetic Acid (EDTA) or α-methyl tyrosine, or exacerbated by pre-treatment with calcium chloride46. EDTA is a sequestering agent for removing Ca2+, a neurotransmitter47; α-methyl tyrosine is a competitive inhibitor for tyrosine in the production of noradrenaline and dopamine48. Pre-treating animals with EDTA or α-methyl tyrosine controlled stress-induced gastric ulcers by reducing neurotransmissions, indicating the CNS was involved into gastric ulceration46. In animal models, gastric ulcers are more effectively induced through manipulating the CNS rather than by altering local factors in the stomach19.
On the other hand, gastric ulcers were found to be a sharply circumscribed loss of tissues in the stomach with a characteristic ‘punch out’ appearance with clean edges12,13. The ‘integral perspective’ derived from the CCR dictates that, all the individual organs in the human body are not independent pieces, but an inseparable integrity20, suggesting that the pathological changes in the stomach may result from the abnormality of other organs21. Multiple modern studies have discovered that the functions of the stomach are under the control of the CNS49,50 (Figure 2a). Thus, the most probable mechanism of gastric ulcers induced in animal models is that the manipulation in the CNS causes pathogenic nerve impulses transmitted to the stomach, leading to gastric ulcers. In duodenal ulcers, what the pathogenic nerve impulses cause is functional changes in the stomach, the hypersecretion of gastric acid21, whereas in gastric ulcers, what the pathogenic nerve impulses cause is structural changes, gastric ulcerations. Once both the pathogenic nerve impulses from the CNS and the morphology of gastric ulcers are considered together, it is natural to speculate that before gastric ulceration, there is a pre-ulcer lesion, which is a node-like aseptic necrotic tissue in the gastric wall (Figure 2b). This deduced psychopathological model is termed ‘submucous node’. Herein the formation of submucous nodes in gastric wall is believed to be a decisive process in gastric ulcerations and the mechanism leading to the morphology, which subsequently determines all the other local characteristics of gastric ulcers in the stomach. Significantly, this psychopathological model is the key to a full understanding of the pathogenesis of peptic ulcers, including providing important clues to the hyper-secretion of gastric acid in duodenal ulcers. Thus, the new etiological theory proposed in the series of 6 articles was termed Theory of Submucous Nodes; briefly Theory of Nodes.
It is noteworthy to mention that in Theory of Nodes, the formation of submucous nodes is caused not by any of the local aggressive factors in the stomach, but by the pathogenic nerve impulses from the CNS. The degree to which individuals suffer negative impacts from life events determines the properties of submucous nodes, such as the size, location, duration, relapse and multiplicity. The formation of submucous nodes might be a rapid process when individuals suffer intense emotional reactions. Strong pathogenic nerve impulses from the CNS may result in severe constriction, cramping, and necrosis of local tissues, and the resulting submucous nodes can be observed in only living patients and may not be found during autopsy. The window for catching the moment when the submucous nodes occur might be very short and currently, all the modern medical techniques are developed to observe the mucosal or serosal sides of the gastric wall, not what happens inside the gastric wall. All these make the submucous nodes too elusive by current laboratory-driven research.
Late phase of gastric ulceration: symptomatic ulcers
Similar to duodenal ulcers, the late phase of gastric ulceration is also a corrosive process caused by the local aggressive factors in the stomach, such as gastric acid and pepsin, H. pylori, mechanical abrasion, NSAIDs and other drug medications (Figure 1h). In healthy individuals, the gastric mucosa is resistant to all the local aggressive factors. However, once submucous nodes have formed in the gastric wall, the blood supply to the local mucosa at the site of the nodes is dramatically decreased. Consequently, the local mucosa’s resistance to aggressive factors in the stomach is remarkably reduced (Figure 2c). Existing data shows that the resistance of the gastroduodenal mucosa to acid digestion depends upon an adequate supply of blood51, and the hypoperfusion of the upper gastrointestinal tract was the major cause of gastrointestinal ulceration52,53. The lower resistance to local aggressive factors leads to necrosis of mucosal layer at the site, and then slough off. Subsequently, the submucous nodes were ejected from the gastric wall due to mechanical extrusion, resulting in the preliminary formation of gastric ulcers (Figure 2d). The process described above indicates that, all the local aggressive factors in the stomach, gastric acid, H. pylori, and NSAIDs, are involved in the pathological process, but in only the late phase of gastric ulceration. Evidently, none of them is a cause of gastric ulcers.
The shape and size of submucous nodes determine the morphology of gastric ulcers. The nodes have a clear border involving the submucosa and muscular layers. As a result, gastric ulcers have a sharply circumscribed loss of tissue involving the mucosa, sub-mucosa, and muscular layer12. Local aggressive factors in the stomach stimulate and corrode the soft tissues around the lesion, causing contraction, denaturation and necrosis. Accordingly, gastric ulcers display a characteristic ‘punch out’ appearance with clean edges, as if it were cut by a knife (Figure 2e). Finally, the tissues around regenerate to rehabilitate the local structure and function (Figure 2f); ulcers heal into scar tissues (Figure 2g).
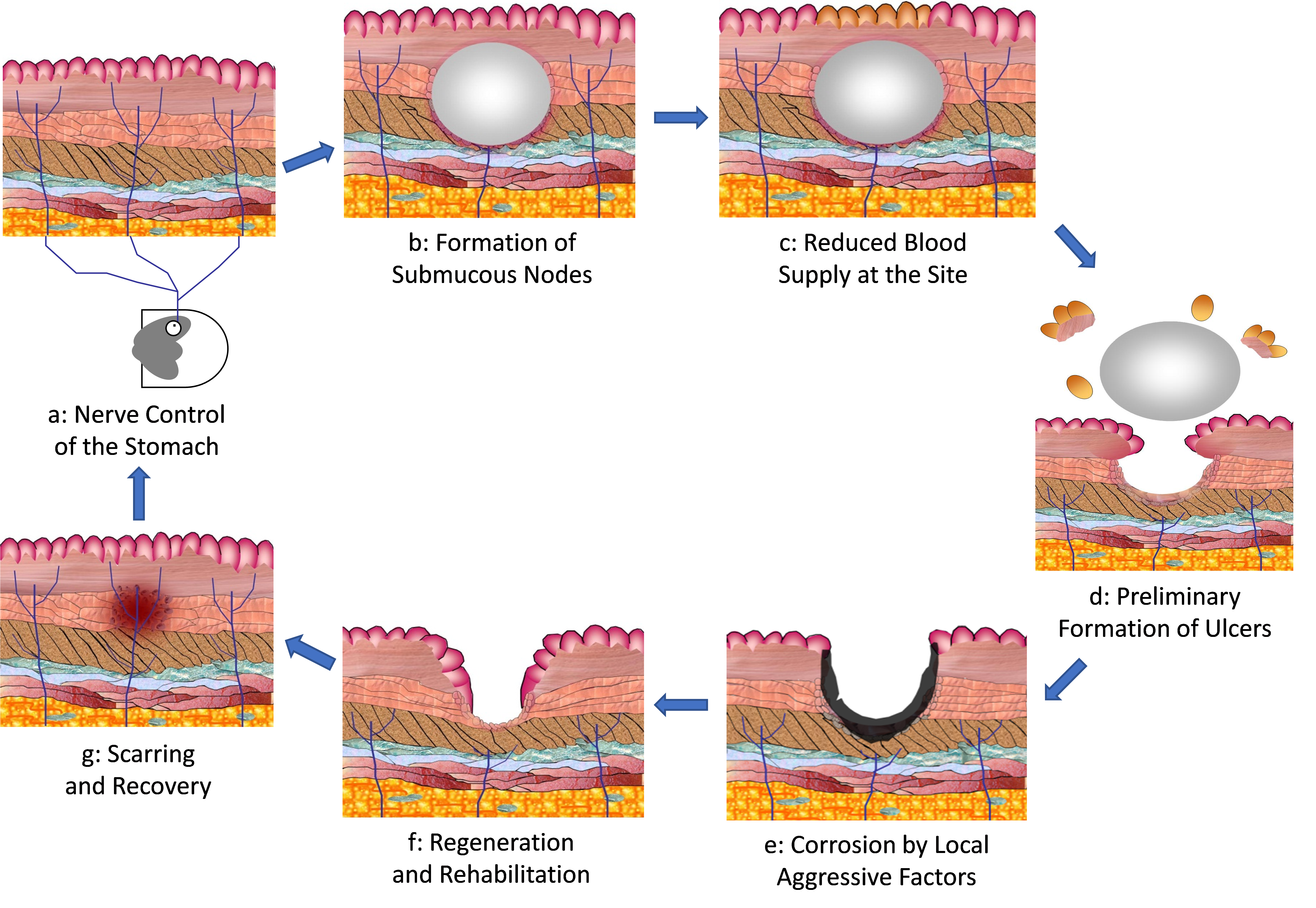
Figure 2: The pathological process of gastric ulceration.
(a) The activities and functions of the stomach are under the control of the CNS. (b) The pathogenic nerve impulses from the CNS cause the formation of submucous nodes in the gastric wall. (c) Submucous nodes block the blood supply to the mucosa at the site, leading to much lower resistance to local aggressive factors in the stomach. (d) Mucosa at the site necrotizes and sloughs off. The submucous nodes are ejected from the gastric wall due to mechanical extrusion. (e) Local aggressive factors stimulate and corrode the tissues around the lesion, causing contraction, denaturation, and necrosis. Ulcer site displays a characteristic ‘punch out’ appearance with clean edges. (f) Tissues around the lesion regenerate to rehabilitate the structure and function. (g) Ulcer heals into scar tissue.
The local characteristics of gastric ulcers
The submucous nodes in the gastric wall account for all the local characteristics and observations/phenomena of gastric ulcers, as well as the roles of gastric acid, H. pylori, and NSAIDs, highlighting the importance of the psychopathological model for a full understanding of the pathogenesis of gastric ulcers. Notably, the mechanisms on some of the characteristics of gastric ulcers elucidated herein are also applicable to duodenal ulcers.
The bleeding and perforation of gastric ulcers
The bleeding and perforation of gastric ulcers are determined by the size and location of submucous nodes. If the nodes are small and superficial, the ulcer will be small and superficial; if the nodes are deep into the serosa, the ulcers will penetrate deep into the serosa. A small node will not penetrate the serosa and rarely results in perforation and the symptoms are less severe. In contrast, a large node may penetrate the serosa, allowing the gastric wall to be perforated when exposed to local aggressive factors. In addition, if large blood vessels are close to the nodes, they may rupture due to the corrosive local aggressive factors, causing bleeding. In Theory of Nodes, the degree to which individuals suffer negative impacts from life events determines the size and depth of the nodes. A moderate stress causes small and superficial ulcers, whereas severe emotional stress may cause ulcer perforation and bleeding56. Therefore, gastric ulcers are not penetrating lesions beginning in the mucosa and extending into the wall of the stomach51, but are primed by the necrotic tissues (nodes) pre-existing within the gastric wall, which make the mucosa highly susceptible to the local aggressive factors.
Self-healing and the effect of clinical treatments
The impacts of the pathogenic nerve impulses are relieved at the ulcerated location once the distal ends of the nerve cells necrotize. As a result, gastric ulcers may heal up automatically via the regeneration of local tissues without treatment57. Animal studies found that aggression gave mice an outlet for their stress, leading to less incidence of gastric ulcerations58. Similarly, gastric ulceration is an outlet for psychological stress in humans. In most cases, especially in those subclinical patients, ulcers may heal up automatically due to the resolution of life events. Unfortunately, the local aggressive factors in the stomach, such as gastric acid and pepsin, H. pylori, NSAIDs, and mechanical abrasions may delay the healing process59. Medications may attenuate the impact of local aggressive factors, such as inhibiting the hyper-secretion of gastric acid, eradicating H. pylori, increasing the resistance of mucosa, or protecting the injured mucosa59. Thus, medications are conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits51,60,61.
The relapse and multiplicity of gastric ulcers
The relapse and multiplicity of nodes determine the relapse and multiplicity of gastric ulcers. As long as the negative impacts of psychosocial factors still exist, the relapse of gastric ulcers will be inevitable. In clinics, medications, such as proton pump inhibitors for gastric acid reduction and antibiotics for H. pylori eradication, may mitigate symptoms, reduce the morbidity rate, and delay relapse to a certain degree, and many cases were diagnosed as healed, but the real cause of gastric ulcers, psychosocial stress, was not removed. Consequently, ulcers may relapse during treatments. Moreover, for individuals with specific personality traits, even trivialities can cause severe impacts and they are more susceptible to life events. Some patients not subject to crucial life events may suffer gastric ulceration due to personality traits that cause emotional trauma and feelings of insecurity51. Long-term effects from past crucial events and specific personality traits explain the relapse of some individuals without suffering immediate crucial events. For example, the loss of family members may lead to chronic emotional stress. As a result, ‘Once an Ulcer, Always an Ulcer’62 is relevant because the true cause, psychological stress, is not relieved by current ulcer medications. In Theory of Nodes, peptic ulcers are a psychosomatic disease triggered by psychological stress, suggesting that the perception of stress determines if a life event can cause ulcer diseases. After repeated exposure to the same stressful life events, the individual may be mentally prepared and respond calmly without perception of stress. Thus, psychologically meaningful experiences may modulate the vulnerability to gastric ulcers and provides some degree of protection against ulcers during the second or later exposures19,63. Multiple hereditary and acquired factors determine the proliferation, differentiation, and distribution of the enteric nervous system64–66. Accordingly, the pathogenic nerve impulses from the CNS may affect the tissues at multiple locations in the stomach simultaneously, causing the multiplicity of submucous nodes in the gastric wall of some individuals. Clinically, the disease manifests as the characteristic of multiplicity.
The roles of gastric acid, pylori, and NSAIDs in gastric ulcers
In modern medicine, gastric acid, H. pylori, and NSAIDs, were considered etiological factors of peptic ulcers one after another, but their roles in the disease were controversial and elusive. In Theory of Nodes, gastric ulceration is determined not by any of the local aggressive factors in the stomach, but by the formation of submucous nodes due to the pathogenic nerve impulses from the CNS. Thus, any one of the local factors in the stomach is not an etiological factor, but a risk factor playing a role in only the late phase of gastric ulceration, exacerbating clinical symptoms and increasing morbidity rates.
The role of gastric acid
Clinical observations found that gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid, and the decreased acid-peptic activity suggests impaired mucosal defence4,5. In Theory of Nodes, gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid, and it is the pre-existed submucous nodes that account for the impaired mucosal defence4,5. In addition, gastric acid secretion in duodenal ulcer patients is much higher than normal, but only 7-8.5% of duodenal ulcer patients concomitantly suffer from gastric ulcers67,68, further indicating that the hypersecretion of gastric acid is not a cause of gastric ulcers. This elucidated why Dragutin Schwartz’s dogma ‘No Acid, No Ulcer’ does not fit gastric ulcers.
The role of H.pylori
In Theory of Nodes, gastric ulceration is determined not by any of the local aggressive factors in the stomach, but by the formation of submucous nodes pre-existing in the gastric wall. Only after the submucous nodes have come into being, could H. pylori have the chance to corrode the tissues at the site, enlarging the lesions and delaying the regeneration and rehabilitation of local tissues. Therefore, H. pylori is a risk factor playing a role in only the late phase of gastric ulceration, exacerbating clinical symptoms, elongating the course of ulcers, and increasing morbidity/mortality rates of gastric ulcers. That explained the observation that ulcer areas in the H. pylori-infected rats were significantly larger than in the uninfected, and ulcer healing was delayed in the infected rats69.
The formation of submucous nodes is irrelevant to H. pylori infection, but determined by only the pathogenic nerve impulses from the CNS. Without infection, gastric ulcers may occur if the individual is severely impacted by psychological stress. Therefore, more than 50% of clinical gastric ulcer patients can be H. pylori-negative16,17,70, and many peptic ulcers were found to be unrelated to the infection of H. pylori, but to other unidentified factors17,18. In Theory of Nodes, the pre-existed pathological lesions in the gastric wall due to psychological stress account for the ‘other unidentified factors’. On the other hand, because gastric ulceration is determined not by H. pylori infection, but by the formation of submucous nodes induced by psychological stress, even though the infection rate in the population is as high as 90%71, only the individuals affected by psychological stress become ulcer patients, leading to ‘the low incidence of gastric ulcers despite a high prevalence of H. pylori infection’15. Since H. pylori infection is not the cause of peptic ulcers, the attempt to explain an epidemiological observation by H. pylori infection would inevitably result in an inconsistency that ‘despite the fall in prevalence of H. pylori infection, the attributable risk of H. pylori infection in peptic ulcer disease has not changed’72.
Notably, in duodenal ulcers, it is the total corrosive intensity of all local aggressive factors that determines the occurrence of ulcerations. As a result, H. pylori density is associated with the morbidity rate of duodenal ulcers73. In contrast, in gastric ulcers it is not the total corrosive intensity of local aggressive factors, but the formation of submucous nodes that determines the occurrence of gastric ulcers. Therefore, H. pylori has a dose-effect on only duodenal ulcers, whereas gastric ulcers’ association with H. pylori is less clear than duodenal ulcers5.
The role of NSAIDs
Similar to H. pylori, NSAIDs are not an etiological factor of peptic ulcers in Theory of Nodes, but a risk factor playing a secondary role in only the late phase of peptic ulcers, exacerbating the clinical symptoms and increasing the morbidity/mortality rates. As stated previously21, in duodenal ulcer it is the hyper-secretions of gastric acid that determines if NSAIDs usage induces duodenal ulcerations, whereas in gastric ulcer it is the pre-existed submucous nodes that determine if NSAIDs usage induces gastric ulcerations. Only the NSAIDs users with hypersecretion of gastric ulcers or pre-existed submucous nodes can become duodenal or gastric ulcer patients. This explains the clinical observation that 14% of long-term NSAIDs users develop gastric ulcers and 10% develop duodenal ulcers74. The absence of hypersecretion of gastric acid and/or formation of submucous nodes explains the majority (86-90%) of NSAIDs users do not develop peptic ulcers74.
Currently, peptic ulcers are classified into H. pylori-related, NSAIDs-related, and idiopathic (Non-H. pylori, non-NSAID) ulcers75. The idiopathic ulcers suggest that other unidentified causative factors may be involved into the pathological process of gastric ulcerations16,72. Without other risk factors, only 0.4% of long-term NSAIDs users develop ulcers, whereas with multiple risk factors (such as bleeding and perforation), 9% of long-term NSAIDs users develop ulcers76,77, suggesting that the vast majority of NSAIDs users will not develop peptic ulcers and other unidentified causative factors determine the occurrence of peptic ulcers. In Theory of Nodes, the ‘other unidentified causative factors’ are elucidated to be the hypersecretion of gastric acid or the pre-existed submucous nodes in the gastric wall.
Since NSAIDs usage is not an etiological factor of peptic ulcers, the etiology based on NSAIDs has inevitably led to controversies and challenges in the field6,7,78, and the classification of peptic ulcers based on H. pylori and NSAIDs does not help to elucidate the pathogenesis of peptic ulcers, but make the pathogenesis of NSAIDs-induced peptic ulcers ‘complex’ or ‘multi-factorial’7,61. In addition, the younger the individuals, the less chances they get infected with H. pylori and/or become NSAIDs users. Thus, ‘there was a significantly higher incidence of idiopathic peptic [duodenal] ulcers in the younger generation’72.
The similarities and differences between duodenal and gastric ulcers
Although duodenal and gastric ulcers share some common features, they are believed to be two different diseases. Duodenal and gastric ulcer patients were found to be epidemiologically, behaviourally, and genetically different12,79. A study compared the inheritance of duodenal and gastric ulcers in 109 families, finding that family members of gastric ulcer patients were more at risk for gastric ulcers, whereas family members of duodenal ulcer patients were more susceptible to duodenal ulcers80. In Theory of Nodes, individuals who are susceptible to gastric and duodenal ulcers belong to two genetically different populations. Noticeably, some individuals may have the genetic background for both gastric and duodenal ulcers and thus, they may have both types of ulcers simultaneously. Gastric ulcer can be induced only in specially bred rat strains19, reflecting the impacts of heredity on the occurrence of the disease. In Theory of Nodes, heredity determines that gastric ulcers can be induced only in 8-30% of mouse models19. Based on the contents in the first and this second articles of the series, Table 1 listed the major similarities and differences between gastric and duodenal ulcers.
Table 1: Similarities and differences between gastric and duodenal ulcers
|
|
Duodenal ulcer |
Gastric ulcer |
|
Similar Features |
1. A psychosomatic disease triggered by stress due to specific personality traits and/or family/social/natural events. |
|
|
2. Brain-driven events with abnormal neurotransmitter release in the CNS. |
||
|
3. The effector organ of abnormal neurotransmitter release is the stomach. |
||
|
4. H. pylori and NSAIDs are risk factors playing a secondary role in only the late phase of ulcerations. Neither H. pylori nor NSAIDs are essential. |
||
|
Different Features |
1. Patients with genetic predisposition for duodenal ulcers. |
1. Patients with genetic predisposition for gastric ulcers. |
|
2. Caused primarily by secondary stressors derived from crucial life events, usually long-term and chronic: laborious work, bad habits and poor work environment. |
2. Caused directly by crucial events, usually short term and acute: wars, unemployment, financial crisis, catastrophe, loss of family members, divorce. |
|
|
3. Chronic stress induced hyperplasia and hypertrophy of gastrin and parietal cells in the stomach in the early phase. |
3. Past life experience developed a negative life-view in the early phase, very subtle functional and structural abnormality in the brain. |
|
|
4. Functional changes induced by psychological stress, resulting in the hypersecretion of gastric acid in the intermediate phase. |
4. Pathological changes in the gastric wall induced by psychological stress, resulting in the formation of submucous nodes in the intermediate phase. |
|
|
5. In the late phase, the total sum of intensities from all aggressive factors determines ulceration. Gastric acid plays a baseline role, where H. pylori or NSAIDs play a secondary role in only the late phase and they also contribute to the final ulcerations. |
5. In the late phase, the formation of submucosal nodes is unrelated to gastric acid, H. pylori, and NSAIDs. All the 3 factors play a role in only the late phase of ulceration. The patients can be hyper-, normo-, or hypo-secretors of gastric acid. |
|
|
6. H. pylori density is associated with the morbidity and mortality rates of duodenal ulcers. |
6. The association between H. pylori and ulceration is weak. |
|
|
7. It is hard to simulate the human condition of chronic stress in lab. Therefore, it is difficult to establish animal models of stress-induced duodenal ulcers. |
7. Animal models can simulate the human condition of acute stress. Therefore, all stress-associated ulcers induced in lab are gastric ulcers. |
|
Discussion
The morphology of gastric ulcer, along with many other characteristics and observations/ phenomena, has remained a mystery for 230 years. Moreover, the roles of gastric acid, H. pylori, and NSAIDs have never been identified before. Herein Theory of Nodes proposed a psychopathological model, submucous nodes in the gastric wall, to elucidate the morphology of gastric ulcers, as well as the other 12 characteristics and 24 observations/phenomena (Supplementary Table S2-S6). This model also identified the roles of gastric acid, H. pylori, and NSAIDs in the disease. Significantly, the similarities and differences between duodenal and gastric ulcers were also clarified. Unequivocally, it is the psychopathological model that garners Theory of Nodes unprecedented insights into gastric ulcers, making a complete cure without relapse possible.
The psychopathological mechanism suggests that similar to duodenal ulcer, gastric ulcer is also a chronic disease associated with past life experience, and stress management is essential for a complete cure of the disease without relapse. This model also suggests that the crux of gastric ulcer issue is the formation of a negative lifeview due to daily life. Clinical medications do not relieve the psychological stress caused by personality traits or life events, and thus cannot effectively prevent the relapse in many patients81. Herein Theory of Nodes recommends two levels of stress management for gastric ulcer control. At the individual level, a positive and optimistic lifeview is the key to significantly improve both physical and mental health. Unequivocally, a harmonious growth environment with proper guidance from parents and/or teachers is crucial to cultivate a positive lifeview of the individual. At the societal level, an equitable, supportive, cooperative, and accepting society will help to cultivate positive life-views and minimize the occurrence of gastric ulcers. By working together as a whole, society can create a healthy external environment that will nurture, grow, support, and sustain a mentally healthy individual. These endeavors will maximally reduce the morbidity and mortality rates of gastric ulcers and thus, fundamentally prevent the disease without relapse.
The data analyses above suggests that the mechanism leading to the morphology of gastric ulcers is a steppingstone to elucidate most of the characteristics and observations/ phenomena of the disease. However, the morphology of gastric ulcers has never been fully elucidated before, causing slow progress in the field over the past centuries. In fact, the finding of Nerve Theory that stress-related gastric lesions are ‘brain-driven’ events, the well-described morphology of gastric ulcers, and the neuroanatomy of the stomach altogether have implicated the pre-existed lesion in the gastric wall, but the pathological model for gastric ulcer has never been proposed in modern medicine. To understand why this model has never been proposed before, Theory of Nodes traced the epistemology of modern medicine back to its historical origin, finding that modern medicine is an evidence-based branch of science, which does not take entities that are undetectable by instruments into consideration and focuses primarily on empirical evidence, such as lab research, clinical observations, or epidemiological surveys82. As a result, the epistemology of modern medicine is fundamentally positivist, a philosophy based on positive facts that can be seen or proven, rather than on ideas derived from sensory experience, interpreted through rational, logical deductions, or mathematical treatments83.
In the case of peptic ulcers, three facts prevented the proposal on a model for gastric ulcer in modern research. First, the technology to inspect the lesions in the interior of the gastric wall of living individuals has not been developed. In current clinical practice, the gastroscopy or laparoscopy can identify existing ulcers, but only in the mucosal or serosal sides of the stomach. Second, the formation of submucous nodes is an acute dynamic process occurring in the living body, which has never been detected because it was beyond the scope of modern research. Third, currently, designing experiments to observe the intermediate process of gastric ulcers is not only challenging but also impossible, because which individuals will be the victims of stressful life events is unpredictable15, and intubation itself may lead to acute stress ulcers84. Consequently, the psychopathological model, submucous node, cannot be observed or detected by any current technique. Committed to empirical evidence, modern researchers discounted this model for elucidating the morphology of gastric ulcers.
Notably, both of the greatest achievements in physics, the Law of Universal Gravitation and the Theory of Relativity, were derived from theoretical deductions, suggesting that tangible experimental studies were not the only way to conduct scientific research and theoretical deductions are also indispensable. The discovery of Neptune in 1846 was not directly by astronomical observations, but by mathematical deductions85, further suggesting the importance of theoretical deductions in scientific research. Interestingly, of all the 81 observations/phenomena of peptic ulcers, the two most challenging topics, the morphology of gastric ulcers (this second article) and the birth-cohort phenomena (the fourth article), were addressed by theoretical deductions in Theory of Nodes, indicating that the major progress of life science and medicine may have to rely heavily on theoretical deductions, especially for those very challenging topics.
Life science and medicine are much more complex than physics and therefore, the routine theoretical deductions are usually inadequate to study life phenomena and human diseases. In the case of peptic ulcer research, a wide variety of topics are associated, including genetics, anatomy, etiology, psychology, epidemiology, neurology, pathology, pathophysiology, bacteriology, clinical observation and statistics, and pre-clinical studies, each of which encompasses multiple subtopics in heterogeneous sources. For example, the single topic of etiology includes 13 historical theories2, making it difficult to find the valuable information for theoretical deduction from tremendous amounts of data accumulated over the centuries. Facing this challenge, the CCR dictates that philosophy can play a guiding role in medical research, which directed Theory of Nodes to locate and incorporate the information for theoretical deduction. First, the CCR directed Theory of Nodes to pinpoint the real cause of peptic ulcers from the 13 etiological theories in history21, thereby disentangling the huge amount of data on peptic ulcers. Second, guided by historical perspective, Theory of Nodes traced the evolution of etiological studies to gain a multidisciplinary view of peptic ulcers. As a result, 4 etiological theories in history (Psychosomatic Theory, Stress Theory, Nerve Theory, and ‘No Acid, No ulcer’), which were deemed outdated after the discovery of H. pylori, were proved useful for a full understanding of peptic ulcers 2. Third, while integral perspective guided Theory of Nodes to combine 5 major etiological theories together21, the gap between the brain-driven events observed in Nerve Theory and the morphology of gastric ulcers explicitly suggested the submucous nodes in the gastric wall and thus, the psychopathological model was proposed to explain the pathogenesis of gastric ulcers. It is worth mentioning that the CCR and its accompanying historical and integral perspectives are philosophical principles. Compared to all the other 13 etiological theories in history, Theory of Nodes is characterized by the application of philosophical principles, thereby proposing the psychopathological model for a full understanding of gastric ulcers. Unequivocally, the effectiveness of this model showcased herein highlighted the guiding role of philosophy in medical research.
Conclusion
Gastric ulcer is a psychosomatic disease triggered by psychological stress, where gastric acid, H. pylori, and NSAIDs play a secondary role in only the late phase of ulcerations, exacerbating clinical symptoms and increasing clinical morbidity/mortality rates. A negative lifeview based on heredity and past life experiences makes the individuals evaluate themselves or current life events negatively, triggering acute psychological stress and the transmission of pathogenic nerve impulses from the CNS to the stomach. The pathogenic nerve impulses cause ‘pre-ulcer lesions’ in the gastric wall, submucous nodes, which significantly reduce the resistance of the mucosa on-site to local aggressive factors in the stomach, eventually resulting in gastric ulcerations. This psychopathological model elucidated 12 characteristics and 24 observations/phenomena of gastric ulcers in this article, suggesting that theoretical research is as important as empirical study in medical explorations. Due to the complexity of life phenomena and human diseases, the application of philosophical principles could prove very beneficial to the research in life science and medicine.
Acknowledgements
Special thanks to Katelynn J. Rowe, who contributed time and effort to challenge the ideas, optimize the structure, and enrich the contents of the article. Many thanks to Douglas Rowe and Dr. Jonathan Weldrick for draft revisions. I would also like to thank Dr. Xiao Xiang and Dr. Stephen Holland for their constructive comments.
Conflict of Interest
The author has no conflict of interest to declare.
Ethics Statement
This study was conducted with integrity, fidelity, honesty, and did not involve any human or animal specimen.
Funding Statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Data Availability Statement
All the supporting data in this article are published papers or books, or in the supplementary materials.
Supplemental Materials
The supplementary materials include 6 tables in a PDF document.
ORCID: Simon Xin Min Dong https://orcid.org/0000-0003-0073-7216
References
- Boles RS. Modern Medical and Surgical Treatment of Peptic Ulcer: An Appraisal. J Am Med Assoc. 1948; 136: 528-535.
- Dong SXM, Chang CCY. Rowe KJA collection of the etiological theories, characteristics, and observations/phenomena of peptic ulcers in existing data. Data Br. 2018; 19: 1058–1067.
- Kuang H. Peptic Ulcer Diseases. (People’s Medical Publishing House, 1990).
- Cho CH. et al. The role of histamine and serotonin in gastric acid secretion: A comparative study in gastric and duodenal ulcer patients. J Gastroenterol Hepatol. 1986; 1: 437–442.
- Huang JQ, Hunt RH. pH, Healing rate and symptom relief in acid-related diseases. Yale J Biol. Med. 1996; 69: 159–174.
- Yeomans ND. The ulcer sleuths: The search for the cause of peptic ulcers. J Gastroenterol. Hepatol. 2011; 26, 35–41.
- Musumba C, Pritchard DM, Pirmohamed M. Review article: cellular and molecular mechanisms of NSAID-induced peptic ulcers. Aliment Pharmacol Ther. 2009; 30: 517–531.
- Marshall BJ. Peptic Ulcer: An Infectious Disease? Hosp Pract. 1987; 22: 87–96.
- Arkkila P. Eradication of Helicobacter pylori improves the healing rate and reduces the relapse rate of nonbleeding ulcers in patients with bleeding peptic ulcer. Am J Gastroenterol. 2003; 98, 2149–2156.
- Hardy J. Helicobacter pylori-Medical Wisdom Challenged by a Cocktail. Jay Hardy, CLS, SM St. Maria, CA. 2016.
- Malfertheiner P, Chan FKL, McColl KEL. Peptic ulcer disease. Lancet 374, 1449–1461 (2009).
- Damon A, Polednak AP. Constitution, genetics, and body form in peptic ulcer: A review. J. Chronic Dis. 20, 787–802 (1967).
- Carton J, Daly R, Ramani P. Clinical Pathology. (Oxford University Press, 2007).
- Konturek SJ, et al. Helicobacter pylori, non-steroidal anti-inflammatory drugs and smoking in risk pattern of gastroduodenal ulcers. Scand. J. Gastroenterol. 38, 923–930 (2003).
- Walsh JH, Peterson WL. The Treatment of Helicobacter pylori Infection in the Management of Peptic Ulcer Disease. N. Engl. J. Med. 333, 984–991 (1995).
- Jones MP. The role of psychosocial factors in peptic ulcer disease: Beyond Helicobacter pylori and NSAIDs. J. Psychosom. Res. 60, 407–412 (2006).
- Kato S, et al. The prevalence of Helicobacter pylori in Japanese children with gastritis or peptic ulcer disease. J. Gastroenterol. 39, 734–738 (2004).
- Elitsur Y, Lawrence Z. Non-Helicobacter pylori related duodenal ulcer disease in children. Helicobacter 6, 239–243 (2001).
- Glavin GB, et al. The neurobiology of stress ulcers. Brain Res. Rev. 16, 301–343 (1991).
- Dong SXM, Chang CCY. Philosophical Principles of Life Science. Wunan Culture Enterprise (Wunan Culture Enterprise, 2012).
- Dong SXM. The hyperplasia and hypertrophy of gastrin and parietal cells induced by chronic stress explain the pathogenesis of duodenal ulcer. J. Ment. Heal. Clin. Psychol. 6, 1–12 (2022).
- Hoksbergen R. Approaches to evaluation of development interventions: The importance of world and life views. World Dev. 14, 283–300 (1986).
- Carey G, DiLalla DL. Personality and psychopathology: Genetic perspectives. J. Abnorm. Psychol. 103, 32–43 (1994).
- Johnson W. Genetic and environmental influences on behavior: Capturing all the interplay. Psychol. Rev. 114, 423–440 (2007).
- Nes RB. Happiness in Behaviour Genetics: Findings and Implications. J. Happiness Stud. 11, 369–381 (2010).
- Feldman M, Walker P, Green JL, etc. Life events stress and psychosocial factors in men with peptic ulcer disease: a multidimensional case-controlled study. Gastroenterology 91, 1370–9 (1986).
- Pratt G. Reflections of an Indigenous Counsellor: Sharing the Journey–Therapist and Person? Australas. Psychiatry 15, S54–S57 (2007).
- Oh S, Chang SJ. Concept Analysis: Family Resilience. Open J. Nurs. 04, 980–990 (2014).
- Van Loon LMA, Van de Ven MOM, Van Doesum KTM, etc. The Relation Between Parental Mental Illness and Adolescent Mental Health: The Role of Family Factors. J. Child Fam. Stud. 23, 1201–1214 (2014).
- Stephan SH, Weist M, Kataoka S, etc. Transformation of children’s mental health services: The role of school mental health. Psychiatr. Serv. 58, 1330–1338 (2007).
- RuževiÄius J. Quality of life and of working life: conceptions and research. 17th Toulon-Verona Int. Conf. Liverpool John Moores Univ. England. 28–29 (2014).
- Walters T, Quinn SR, Walters LM. Media life among Gen Zeds. Int. J. Cult. Stud. 8, 63–82 (2005).
- Goubert L, Vlaeyen JWS, Crombez G, etc. Learning About Pain From Others: An Observational Learning Account. J. Pain 12, 167–174 (2011).
- Lim C, Putnam RD. Religion, Social Networks, and Life Satisfaction. Am. Sociol. Rev. 75, 914–933 (2010).
- Bektas Ä°, KudubeÅ AA, Ayar D, etc. Predicting the Healthy Lifestyle Behaviors of Turkish Adolescents Based on their Health Literacy and Self-Efficacy Levels. J. Pediatr. Nurs. 59, e20–e25 (2021).
- Kim J, Lee SW, Kwak M, etc. Attitudes Formation by Small but Meaningful Personal Information. Psychiatry Investig. 14, 298 (2017).
- Lerner JS, Keltner D. Beyond valence: Toward a model of emotion-specific influences on judgement and choice. Cogn. Emot. 14, 473–493 (2000).
- Kurata JH, Nogawa AN, Abbey DE, etc. A prospective study of risk for peptic ulcer disease in seventh-day adventists. Gastroenterology 102, 902–909 (1992).
- Starcke K, Wiesen C, Trotzke P, etc. Effects of Acute Laboratory Stress on Executive Functions. Front. Psychol. 7, 1–8 (2016).
- Brouwer AM, Hogervorst MA. A new paradigm to induce mental stress: the Sing-a-Song Stress Test (SSST). Front. Neurosci. 8, 1–8 (2014).
- Susser M, Stein Z. Civilization and Peptic Ulcer. Lancet 279, 116–119 (1962).
- Levenstein S, Rosenstock S, Jacobsen RK, etc. Psychological stress increases risk for peptic ulcer, regardless of helicobacter pylori infection or use of nonsteroidal anti-inflammatory drugs. Clin. Gastroenterol. Hepatol. 13, 498-506.e1 (2015).
- Levenstein S. Stress and peptic ulcer: life beyond helicobacter. Bmj 316, 538–541 (1998).
- Ellard K, Beaurepaire J, Jones M, etc. Acute and chronic stress in duodenal ulcer disease. Gastroenterology 99, 1628–1632 (1990).
- Henke PG. The centromedial amygdala and gastric pathology in rats. Physiol. Behav. 25, 107–112 (1980).
- Sutoo D, Akiyama K, Matsui A. Gastric ulcer formation in cold-stressed mice related to a central calcium-dependent-dopamine synthesizing system. Neurosci. Lett. 249, 9–12 (1998).
- Allen B. Clarkson and Babatunde O. Amole. Role of Calcium in Trypanocidal Drug Action. Sci. New Ser. 216, 1321–1323 (1982).
- Major CT, Pleuvry BJ. Effects of α-methyl-p-tyrosine, p-chlorophenylalanine, l-β-(3,4-dihydroxyphenyl)alanine, 5-hydroxytryptophan and diethyldithiocarbamate on the analgesic activity of morphine and methylamphetamine in the mouse. Br. J. Pharmacol. 42, 512–521 (1971).
- Browning KN, Travagli RA. Central Nervous System Control of Gastrointestinal Motility and Secretion and Modulation of Gastrointestinal Functions. in Comprehensive Physiology 4, 1339–1368 (Wiley, 2014).
- Hernandez DE. Neurobiology of brain-gut interactions. Implications for ulcer disease. Dig. Dis. Sci. 34, 1809–1816 (1989).
- Kirsner JB, Palmer WL. Seminars on gastrointestinal physiology: The problem of peptic ulcer. Am. J. Med. 13, 615–639 (1952).
- Spirt MJ. Stress-related mucosal disease: Risk factors and prophylactic therapy. Clin. Ther. 26, 197–213 (2004).
- Chung SCS, Sung JY, Suen MWM, etc. Endoscopic assessment of mucosal hemodynamic changes in a canine model of gastric ulcer. Gastrointest. Endosc. 37, 310–314 (1991).
- Smout AJPM, Akkermans LMA, Reid K. Normal and Disturbed Motility of the Gastrointestinal Tract. Neurogastroenterol. Motil. 5, 230 (1993).
- Christensen J, Rick GA, Robison BA, etc. Arrangement of the myenteric plexus throughout the gastrointestinal tract of the opossum. Gastroenterology 85, 890–899 (1983).
- Peters MN, Richardson CT. Stressful Life Events, Acid Hypersecretion, and Ulcer Disease. Gastroenterology 84, 114–119 (1983).
- Feldman M, Weinberg T. Healing of peptic ulcer. Am. J. Dig. Dis. 18, 295–6 (1951).
- Tanaka T, Yoshida M, Yokoo H, etc. Expression of aggression attenuates both stress-induced gastric ulcer formation and increases in noradrenaline release in the rat amygdala assessed by intracerebral microdialysis. Pharmacol. Biochem. Behav. 59, 27–31 (1998).
- Tarnawski A. Cellular Mechanisms of Gastric Ulcer Healing. in The Stomach 177–192 (Springer Berlin Heidelberg, 1993).
- Samonina GE, et al. Antiulcer effects of amylin: A review. Pathophysiology 11, 1–6 (2004).
- Schmassmann A. Mechanisms of Ulcer Healing and Effects of Nonsteroidal Anti-inflammatory Drugs. Am. J. Med. 104, 43S-51S (1998).
- Earnest DL. Maintenance Therapy in Peptic Ulcer Disease. Med. Clin. North Am. 75, 1013–1038 (1991).
- Bruce Overmier J, Murison R. Anxiety and helplessness in the face of stress predisposes, precipitates, and sustains gastric ulceration. Behav. Brain Res. 110, 161–174 (2000).
- Heanue TA, Pachnis V. Enteric nervous system development and Hirschsprung’s disease: advances in genetic and stem cell studies. Nat. Rev. Neurosci. 8, 466–479 (2007).
- Stilling RM, Dinan TG, Cryan JF. Microbial genes, brain & behaviour-epigenetic regulation of the gut-brain axis. Genes, Brain Behav. 13, 69–86 (2014).
- Cryan JF, et al. The Microbiota-Gut-Brain Axis. Physiol. Rev. 99, 1877–2013 (2019).
- Johnson HD. The special significance of concomitant gastric and duodenal ulcers. Lancet 265, 266–270 (1955).
- Kameyama J, Sasaki I, Imamura M, etc. Selection of operation for concomitant gastric and duodenal ulcers. Jpn. J. Surg. 13, 16–19 (1983).
- Li H, KALIES I, MELLGÅRD B, etc. A Rat Model of Chronic Helicobacter pylori Infection: Studies of Epithelial Cell Turnover and Gastric Ulcer Healing. Scand. J. Gastroenterol. 33, 370–378 (1998).
- Freston JW. Role of proton pump inhibitors in non-H. pylori-related ulcers. Aliment. Pharmacol. Ther. 15, 2–5 (2001).
- Konturek P. Pioglitazone, a specific ligand of peroxisome proliferator-activated receptor-gamma, accelerates gastric ulcer healing in rat. Eur. J. Pharmacol. 472, 213–220 (2003).
- Quan C, Talley NJ. Management of peptic ulcer disease not related to Helicobacter pylori or NSAIDs. Am. J. Gastroenterol. 97, 2950–2961 (2002).
- Rauws EAJJ, Tytgat GNJJ. Helicobacter pylori in duodenal and gastric ulcer disease. Baillieres. Clin. Gastroenterol. 9, 529–547 (1995).
- Hudson N, Hawkey CJ. Non-steroidal anti-inflammatory drug-associated upper gastrointestinal ulceration and complications. Eur. J. Gastroenterol. Hepatol. 5, 412–419 (1993).
- Sivri B. Trends in peptic ulcer pharmacotherapy. Fundam. Clin. Pharmacol. 18, 23–31 (2004).
- Drina M. Peptic ulcer disease and non-steroidal anti-inflammatory drugs. Aust. Prescr. 40, 91–93 (2017).
- Baigent C, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet 382, 769–779 (2013).
- Gisbert JP, Calvet, X. Review article: Helicobacter pylori-negative duodenal ulcer disease. Aliment. Pharmacol. Ther. 30, 791–815 (2009).
- Susser M. Peptic Ulcer: Rise and Fall. Christie DA, Tansey EM (eds). Wellcome Witnesses to Twentieth Century Medicine. Vol.14, 2002. London: The Wellcome Trust Centre for the History of Medicine, 2002, £10.00 ISBN: 0-85484-084-2. Int. J. Epidemiol. 32, 674–675 (2003).
- Doll R, Kellock TD. The Separate Inheritance of Gastric and Duodenal Ulcers. Ann. Eugen. 16, 231–240 (1951).
- Wong GLH, et al. High Incidence of Mortality and Recurrent Bleeding in Patients With Helicobacter pylori-Negative Idiopathic Bleeding Ulcers. Gastroenterology 137, 525–531 (2009).
- Röhrig B, Prel JB du, Wachtlin D, etc. Types of Study in Medical Research. Dtsch. Aerzteblatt Online 106, 262–268 (2009).
- Caldwell BJ. Beyond positivism: Economic methodology in the twentieth century. (Routledge, 2015).
- Smith R, Perkins N, Firth E, etc. Arytenoid mucosal injury in young Thoroughbred horses—investigation of a proposed aetiology and clinical significance. N. Z. Vet. J. 54, 173–177 (2006).
- Jones HS. John Couch Adams and the discovery of Neptune. (Cambridge University Press, 2014).
Supplementary Materials
Table S1: List of 6 articles to explain all the 15 characteristics and 81 observations/phenomena of peptic ulcers
|
Article |
Title |
|
A1 |
The Hyperplasia and Hypertrophy of Gastrin and Parietal Cells Induced by Chronic Stress Explain the Pathogenesis of Duodenal Ulcers. Published on Journal of Mental Health & Clinical Psychology, 2022, 6(3): 1-12. |
|
A2* |
A Novel Psychopathological Model Explains the Pathogenesis of Gastric Ulcers |
|
A3 |
Painting a Complete Picture of the Pathogenesis of Peptic Ulcers |
|
A4 |
Novel Data Analyses Explain the Birth-Cohort Phenomenon of Peptic Ulcers |
|
A5 |
Novel Data Analyses Explain the Seasonal Variations of Peptic Ulcers |
|
A6 |
Novel Data Analyses Address the African Enigma and The Controversies Surrounding the Roles of Helicobacter Pylori in Peptic Ulcers |
Note: 1. A1: Article 1. 2. * This Article. 3. The 6 articles altogether explained all of the 15 major characteristics and 81 observations/phenomena of peptic ulcers. 4. The order and titles of articles might be modified during publication process.
Table S2: Index of 14 elucidated characteristics of peptic ulcers
|
Classification |
Characteristics |
Explanation in the Article |
Article, Page, Column & Line # |
|
General (3) |
1) Genetic predisposition |
Individuals who are susceptible to gastric and duodenal ulcers belong to two genetically different populations. Notably, some individuals may have the genetic background for both gastric and duodenal ulcers and thus, they may have both types of ulcers simultaneously. |
Article 2, Page 20, Left Column, Lines 14-24. |
|
2) Etiology |
Peptic ulcers are not an infectious disease caused by the H. pylori infection, but a psychosomatic disease triggered by psychological stress. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
|
3) Epidemiology |
|
|
|
|
Clinical symptoms (6) |
4) Predilection sites |
The gastric antrum and lesser curvature have the most complicated function with the largest ganglions and the greatest density of highly developed nerve plexus, determining that the local tissues at these sites receive stronger and more frequent pathogenic nerve impulses from the CNS. |
Article 2, Page 17, Right Column, Line 17-Page 18, Left Column, Line 6. |
|
5) Morphology |
The shape and size of submucous nodes determine the morphology of gastric ulcers. The nodes have a clear border involving the submucosa and muscular layers, determining gastric ulcers have a sharply circumscribed loss of tissue involving the mucosa, sub- mucosa, and muscular layer. Local aggressive factors in the stomach stimulate and corrode the soft tissues around the lesion, causing contraction, denaturation and necrosis. Accordingly, gastric ulcers display a characteristic ‘punch out’ appearance with clean edges. (Figure 1A-G). |
Article 2, Page 17, Left Column, Line 47-Right Column, Line 30. |
|
|
6) Bleeding |
If large blood vessels are close to the nodes, they may rupture due to the corrosive local aggressive factors, causing bleeding. |
Article 2, Page 18, Left Column, Lines 8-28. |
|
|
7) Perforation |
A small node will not penetrate the serosa and rarely results in perforation and the symptoms are less severe. In contrast, a large node may penetrate the serosa, allowing the gastric wall to be perforated when exposed to local aggressive factors. |
Article 2, Page 18, Left Column, Lines 8-28. |
|
|
8) Relapse |
Clinical patients suffer relapses of peptic ulcers because neither anti- secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
|
9) Multiplicity |
The pathogenic nerve impulses from the CNS may affect the tissues at multiple locations in the stomach simultaneously due to the local nerve distribution, causing the multiplicity of submucous nodes in the gastric wall. Clinically, the disease manifests itself as the characteristic of multiplicity. |
Article 2, Page 18, Right Column, Lines 32-39. |
|
|
Local aggressive factors (3) |
10) Gastric acid |
The hypersecretion of gastric acid is an intermediate process of duodenal ulceration, suggesting it is not a cause of duodenal ulcers, but an effect of stress triggered by personality traits or life events. Nevertheless, the hypersecretion of gastric acid is a determinant factor in the late phase of duodenal ulceration, governing many characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-35. |
|
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Gastric acid plays a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 19, Left Column, Lines 2-16. |
||
|
11) H. pylori |
H. pylori infection is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left Column, Line 17; Article 1, Page 7, Right Column, Lines 34-41. |
|
|
H. pylori plays a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 19, Left Column, Line 18-Right Column, Line 12. |
||
|
12) NSAIDs |
NSAIDs usage is not an etiological factor/a cause of duodenal ulcer, but plays a secondary role in only the late phase of ulceration, exacerbating clinical symptoms and increasing the clinical morbidity/mortality of the disease. |
Article 1, Page 2, Right Column, Line 49-Page 3, Left Column, Line 17; Article 1, Right Column, Page 7, Lines 34-41. |
|
|
NSAIDs are not an etiological factor of peptic ulcers in Theory of Nodes, but a risk factor playing a secondary role in only the late phase of peptic ulcers, exacerbating the clinical symptoms and increasing the clinical morbidity/mortality rates. |
Article 2, Page 19, Right Column, Lines 14-30. |
||
|
Prognosis (3) |
13) Self-healing |
In most cases, especially in those subclinical patients, ulcers heal up automatically due to the resolution of life events. Unfortunately, the local aggressive factors in the stomach, such as gastric acid and pepsin, the infection of H. pylori, NSAIDs, and mechanical abrasions may delay the healing process. |
Article 2, Page 18, Left Column, Lines 30-49. |
|
14) Effects of clinical treatments |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, but the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori-negative Cases D and F, or in the H. pylori-positive Cases J and R. Cases like Cases D, F, J and R explains a dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
|
Medications may attenuate the impact of local aggressive factors, such as inhibiting the hyper-secretion of gastric acid, eradicating H. pylori, increasing the resistance of the mucosa, or protecting the injured mucosa. Thus, medications may be conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 18, Left Column, Lines 42-49. |
||
|
15) Hospitalization rates, morbidity, and mortality |
Neither H. pylori infection nor NSAIDs usage is an etiological factor. Both play a secondary role in only the late phase of duodenal ulceration, exacerbating clinical symptoms and increasing clinical morbidity and mortality rates. |
Article 1, Page 7, Right Column, Lines34-41. |
|
|
Gastric acid, H. pylori, and NSAIDs play a role in only the late phase of ulcerations, enlarging the local lesions, exacerbating clinical symptoms, and increasing clinical morbidity/mortality rates. |
Article 2, Page 18, Right Column, Lines 42-52. |
Note: The blank will be filled in other articles of the series.
Table S3: Index of 6 elucidated duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
1. No Acid, No Ulcer (True statement for duodenal ulcer). |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDS. |
Article 1, Page 5, Right Column, Lines 28-34. |
|
2. The role of gastric acid in the pathogenesis of duodenal ulcer is further supported by the relief of pain observed after neutralization or buffering of gastric contents with alkali or food. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors. Thus, neutralization or buffering of gastric contents with alkali or food results in the relief of pain in duodenal ulcer patients. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
3. Doll and Jones’ survey suggested a positive correlation between stressful occupations and duodenal ulcer, a decreased incidence of ulcer among agricultural workers. |
Psychosomatic factors such as hypochondriasis, a negative perception of life events, dependency, and lowered self- confidence, made ulcer patients more susceptible to stress than controls. |
Article 1, Page 3, Right Column, Line 36-Page 4, Left Column, Line 9. |
|
4. Studies suggest that severe anxiety caused acid hypersecretion which, in turn, contributed to ulceration and symptoms. The fact that acid hypersecretion and symptoms abated with alleviation of stress supports this hypothesis. |
The hypersecretion of gastric acid is triggered by the perception of stress via vagus nerves, and the hyperplasia and hypertrophy of gastrin and parietal cells in the early phase significantly potentiated the individual’s response to life events. |
Article 1, Page 5, Left Column, Lines 37-43. |
|
5. Rates of recurrence in patients whose initial ulcers healed during conventional anti-secretory therapy range from 60 to 100 percent per year. |
Neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
6. Duodenal ulcer had higher incidence in large cities compared to rural areas in Africa since the 1950’s. |
Life in large cities is more competitive and stressful than in rural areas. |
Article 1, Page 4, Left Column, Lines 9-12. |
Table S4: Index of 9 elucidated gastric ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
7. No Acid, No Ulcer (wrong statements for gastric ulcers). |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
8. In contrast to patients with duodenal ulcer, most patients with gastric ulcer are normo- secretors or hypo-secretors. Decreased acid-peptic activity in these patients suggests impaired mucosal defence. |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid, and it is the pre-existed submucous nodes that account for the impaired mucosal defence. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
9. Gastric ulcer is a sharply circumscribed loss of tissue involving the mucosa, submucosa, and muscular layer and a characteristic “punch out” appearance with clean edges, as if it were cut by a knife. |
The shape and size of submucous nodes determine the morphology of gastric ulcers. The nodes have a clear border involving the submucosa and muscular layers. As a result, gastric ulcers have a sharply circumscribed loss of tissue involving the mucosa, sub-mucosa, and muscular layer. Local aggressive factors in the stomach stimulate and corrode the soft tissues around the lesion, causing contraction, denaturation and necrosis. Accordingly, gastric ulcers display a characteristic ‘punch out’ appearance with clean edges, as if it were cut by a knife (Fig.1B-F). |
Article 2, Page 17, Right Column, Lines 19-30. |
|
10. Gastric ulcers can be induced only in 8-30% of mouse models. |
In addition, gastric ulcer can be induced only in specially bred rat strains, reflecting the impacts of heredity on the occurrence of the disease. In Theory of Nodes, heredity determines that gastric ulcers can be induced only in 8-30% of mouse models. |
Article 2, Page 20, Left Column, Lines 14-27. |
|
11. Gastric ulceration begin in the mucosa and extend into the wall of the stomach. |
Wrong statement. Gastric ulcers are not penetrating lesions beginning in the mucosa and extending into the wall of the stomach, but are ‘primed’ by the necrotic tissues (nodes) pre-existing within the gastric wall, which make the mucosa highly susceptible to the local aggressive factors. |
Article 2, Page 18, Left Column, Lines 19-28. |
|
12. Stress-related gastric lesions are ‘brain- driven’ events that may be more effectively managed through central manipulations than by altering local, gastric factors. For example, stimulation or lesions of the central nucleus of the amygdala produced or reduced gastric ulcers, respectively. |
The consequence of psychological stress in gastric ulcers is the abnormal release of neurotransmitters in the CNS, leading to the transmission of pathogenic nerve impulses to the stomach. Notably, in Theory of Nodes, what Nerve theory discovers is the intermediate phase of peptic ulcerations. (Please refer to A1) |
Article 2, Page 16, Left Column, Line 23-Right Column, Line 18. |
|
13. Development of gastric ulcers elicited by cold stress was significantly decreased by i.p. pre-treatment with EDTA or α-methyl tyrosine, which depleted neurotransmitters. Gastric ulcers were significantly increased by pre-treatment with CaCl2. |
The consequence of psychological stress in gastric ulcers is the abnormal release of neurotransmitters in the CNS, leading to the transmission of pathogenic nerve impulses to the stomach. EDTA is a sequestering agent for removing a neurotransmitter, Ca2+; α-methyl tyrosine is a competitive inhibitor for tyrosine in the production of noradrenaline and dopamine. Pre-treating animals with EDTA or α-methyl tyrosine-controlled stress-induced gastric ulcers by reducing neurotransmissions. |
Article 2, Page 16, Left Column, Line 23-Right Column, Line 18. |
|
14. The predilection sites of gastric ulcers are gastric antrum and lesser curvature. |
The gastric antrum and lesser curvature have the most complicated function with the largest ganglions and the greatest density of highly developed nerve plexus. Thus, the gastric antrum and lesser curvature are the predilection sites of gastric ulcers. |
Article 2, Page 17, Right Column, Line 41-Page 18, Left Column, Line 6. |
|
15. Vulnerability to gastric ulceration is modulated by psychologically meaningful experiences. Repeated stress of the same type generally, but not exclusively, provides some degree of protection against ulcer during the second or later exposures. |
Peptic ulcer is a psychosomatic disease triggered by psychological stress, indicating that the perception of stress determines if life events cause ulcer diseases. After repeated exposure to the same stressful life events, the individual may be mentally prepared and respond calmly without the perception of stress. Thus, psychologically meaningful experiences can modulate the vulnerability to gastric ulcers and provides some degree of protection against ulcer during the second or later exposures. |
Article 2, Page 18, Right Column, Lines 22-39. |
Table S5: Index of 19 elucidated both gastric and duodenal ulcer-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column &Line # |
|
16. The pathogenesis of NSAID-induced peptic ulcers is complex and multi-factorial. |
A statement based on a wrong etiology. Since NSAIDs usage is not an etiological factor of peptic ulcers, the etiology based on NSAIDs has inevitably led to controversies and challenges in the field, and the classification of peptic ulcers based on H. pylori and NSAIDs does not help to elucidate the pathogenesis of peptic ulcers, but make the pathogenesis of NSAIDs-induced peptic ulcers ‘complex’ or ‘multi-factorial’. |
Article 2, Page 19, Right Column, Lines 45-51. |
|
17. 14% of patients taking NSAIDs chronically can be found to have lesions described as gastric ulcers and 10% have lesions describes as duodenal ulcers. |
In duodenal ulcer, it is the hyper-secretions of gastric acid that determines if NSAIDs usage induces duodenal ulcerations, whereas in gastric ulcer it is the pre-existed submucous nodes that determine if NSAIDs usage induces gastric ulcerations. Only the NSAIDs users with the hypersecretion of gastric ulcers or the pre-existed submucous nodes can become duodenal or gastric ulcer patients. |
Article 2, Page 19, Right Column, Lines 14-30. |
|
18. Birth-cohort Phenomenon: the mortality rate of gastric ulcers in England and Wales increased at the beginning of the 20th century, reached a peak and then began to fall in the early 1950s. They also found similar trends for duodenal ulcers but followed approximately five years behind. |
|
|
|
19. Once an ulcer, always an ulcer. |
Clinical patients suffer relapses of peptic ulcers because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the hyperplasia and hypertrophy of gastrin and parietal cells and the impact of stress have not been eliminated. The pre-existing hyperplasia and hypertrophy and the perception of stress from time to time, resulting in ‘once an ulcer, always an ulcer’. |
Article 1, Page 8, Right Column, Lines 7-14. |
|
20. Seasonal occurrence of peptic ulcer diseases. |
|
|
|
21. Patients free of ulcer distress for long periods of time were subjected to emotional trauma and feelings of insecurity during the symptom-free intervals. |
For individuals with specific personality traits, even trivialities may cause severe impacts and they are more susceptible to life events. Some patients not subject to crucial life events may still suffer gastric ulceration due to personality traits that cause emotional trauma and feelings of insecurity. Long-term effects from past crucial events and specific personality traits explain the relapse of some individuals without suffering immediate crucial events. |
Article 2, Page 18, Right Column, Lines 10-15. |
|
22. Investigations of the effects of perceived stress on physiological parameters are scarce and the findings are often conflicting. |
Questionnaire-based epidemiological surveys may have discounted many chronic stressors during peptic ulcer research, and that the essential methodology to study psychosocial factors (the abstract essence of the human body) have not been established in modern medicine. |
Article 1, Page 5, Left Column, Line 44-Page 6, Right Column, Line 13. |
|
23. There is no definitive study proving a causal relationship between psychological stress and the development of ulcer disease. |
1. Without the CCR, there is no benchmark to identify the cause of ulcer disease. 2. without the methodological concepts derived from the CCR, much invaluable historical data is deemed outdated and remains unanalyzed. |
Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
24. Feldman’s multidimensional case-controlled study found that ulcer patients exhibited significantly more emotional distress in the form of depression and anxiety. Hypochondriasis, a negative perception of their life events, dependency, and lowered self-confidence were the four variables that best discriminated ulcer patients from controls. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2. Right Column, Lines 30-48. |
|
25. Peptic ulcers are a rare disease in childhood. |
|
|
|
26. Although gastric ulcer and duodenal ulcer share something in common, they are believed to be different diseases. |
Individuals who are susceptible to gastric and duodenal ulcers belong to two genetically different populations. Table-1 fully elucidated the similarity and differences between duodenal and gastric ulcers. |
Article 2, Page 20, Left Column, Lines 6-27. |
|
27. The final stage of ulceration is a corrosive rather than an infectious process. |
The late phase of duodenal ulcers is a corrosive process caused by local aggressive factors, including gastric acid and pepsin, H. pylori, mechanical abrasion, and chemical erosion from medications such as NSAIDs. |
Article 1, Page 5, Right Column, Lines 15-34. |
|
28. The gastric acid secretion of duodenal ulcer patients is much higher than a normal person, but only 7–8.5% of the duodenal ulcer patients are suffering from gastric ulcer simultaneously. |
Gastric ulceration is determined not by gastric acid, but by the formation of submucous nodes in the gastric wall. Therefore, gastric ulcer patients can be hypo-, normo-, or hyper-secretors of gastric acid. Some individuals may have the genetic background for both gastric and duodenal ulcers and thus, they may have both types of ulcers simultaneously. |
Article 2, Page 19, Left Column, Lines 2-16. |
|
29. Severe emotional stress may contribute to ulcer perforation and bleeding in some patients. |
The degree to which individuals suffer negative impacts from life events determined the size and depth of the nodes. A moderate stress causes small and superficial ulcers, but severe emotional stress may cause ulcer perforation and bleeding. |
Article 2, Page 18, Left Column, Lines 19-28. |
|
30. Many uncomplicated lesions heal in spite of the presence of acid gastric content, as shown by the “spontaneous” remissions of the disease and by the healed scars found at x-ray and at autopsy; however, the healing of peptic ulcer is much more rapid when the lesion is protected from the action of acid gastric juice. |
The impacts of the pathogenic nerve impulses are relieved at the ulcerated location once the distal ends of the nerves necrotize. As a result, gastric ulcers may heal up automatically via the regeneration of local tissues without treatment. Medications may attenuate the impact of local aggressive factors, such as inhibiting the hyper-secretion of gastric acid, eradicating H. pylori, increasing the resistance of the mucosa, or protecting the injured mucosa. Thus, medications may be conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 18, Left Column, Lines 30-49. |
|
31. Autopsy reports showed: 20%-29% of males and 11%-18% of females were found to have suffered from ulcers in the past or present. |
|
|
|
32. It is believed that, not only should the prognosis and assessment of ulcer have mental assessment, but the treatment without mind adjustment is also incomplete. |
|
|
|
33. Peptic ulcer patients may have “ulcer personality”, such as immaturity, impulsivity, and feelings of social isolation and alienation. |
|
|
|
34. In a 2-year study of Pima Indians, Hesse did not find any peptic ulcer disease. |
|
|
|
35. In contrast to Pima Indians, 10% of Caucasians develop peptic ulcers. |
|
|
|
36. To date, no consistent pattern of factors, in either host or organism, has been identified that successfully predicts which infected persons will subsequently have ulcer disease. |
|
|
|
37. The relationship between life events stress, psychological factors and peptic ulcer diseases is not clearly established at the present time and warrants further study. |
Without the CCR, there is no benchmark to identify the cause of disease. As a result, no disease has been fully understood. Without the CCR, the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. |
Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
38. Richard emphasized the different aetiology of gastric and duodenal ulcers and persons with gastric and duodenal ulcers differ epidemiologically, behaviourally, and genetically. |
Table 1 listed all the commonalties and differences between duodenal and gastric ulcers. |
Article 2, Page 20, Table 1. |
|
39. Gastric ulcer was more frequent than duodenal ulcer, 4G:1D in 1900 versus 10D:1G currently. More women than men had the disease, but now it has become reversed; from 3F:1M to 4M:1F for gastric ulcer and 10M:1F for duodenal ulcer. |
|
|
|
40. Stress ulcers in the rat are primarily gastric rather than duodenal, the latter typically requiring additional artificial chemical potentiation (e.g., histamine). |
It may take ~5 years to induce the hyperplasia and hypertrophy in the human body. As a result, it is hard to duplicate this chronic pathophysiological process in the lab, thereby making it difficult to establish animal models for stress-induced duodenal ulcers. Duodenal ulcer is a chronic disease associated with the individual’s daily behaviors, and multiple psycho-neuro-endocrine organs were involved. Thus, stress induced duodenal ulcer is hardly reproduced in animal models due to short lifespans. |
Article 1, Page 5, Left Column, Lines 14-20; Article 1, Discu, Page 9, Left Column, Lines 15-20. |
|
The psychological stress triggering gastric ulcers is usually short-term and acute. This kind of stress can be simulated in labs and therefore, stress-induced ulcers in labs are usually gastric ulcers. |
Article 2, Page 16, Left Column, Lines 2-11. |
|
|
41. Many ulcer patients and some physicians believe that symptomatic exacerbations of peptic ulcer disease occur during or shortly after stressful events. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
42. Mental disorders (or stress) are associated with increased rates of peptic ulcer diseases. |
Peptic ulcers are a psychosomatic disease triggered by psychological stress. psychosomatic factors, which focuses more on the impact of mental health related to past life experience, made individuals susceptible to psychological stress caused by current life events, leading to peptic ulceration. |
Article 1, Page 2, Right Column, Lines 30-48. |
|
43. The spontaneous remissions and relapses of peptic ulcers have never been explained. |
Clinical patients suffer the relapse of peptic ulcers, because neither anti-secretory nor anti-H. pylori therapy is an etiological treatment and thus, the impact of stress caused by personality traits or negative life events has not been eliminated. Chronic stress-induced hyperplasia and hypertrophy of gastrin and parietal cells are the crux of duodenal ulcer issue, determine the spontaneous remissions and relapse of duodenal ulcer, but this psychopathological mechanism has never been elucidated in modern medicine. The etiology of peptic ulcer has never been identified, causing the problem. |
Article 1, Page 8, Right Column, Lines 7-14; Article 1, Discu, Page 9, Left Column, Lines 15-26. |
|
44. The pathophysiology of peptic ulcer has centred on an imbalance between aggressive and protective factors. |
|
|
|
45. No single theory in history could fully explain the pathogenesis of peptic ulcers. |
Each of the single theory focused on only one area of the human body, and there is no holistic review of peptic ulcers before. Without the CCR, there is no benchmark to identify the true cause of disease. In addition, without the CCR, the methodologies for data analysis have never been established. Although each of the historical theory did make important discoveries and proved useful to understand peptic ulcers, they were overshadowed by the discovery of H. pylori. |
Article 1, Page 3, Left Column, Lines 20-29; Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
Table S6: Index of 30 elucidated H. pylori-related observations/phenomena
|
Observations/phenomena |
Explanation in the Article |
Article, Page, Column & Line # |
|
46. African Enigma: The H. pylori infection rate is high (close to 100%) throughout Africa, but the prevalence of duodenal ulcer varied in different parts of the continent. |
|
|
|
47. Only the presence of duodenal ulcers, and not gastric ulcers, was associated with increasing H. pylori density. The association between gastric ulcers and H. pylori infection is less clear. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. Cases B to J explain why H. pylori density is associated with the morbidity rate of duodenal ulcers. |
Article 1, Page 7, Right Column, Lines 34-48. |
|
In gastric ulcers, it is not the total corrosive intensity of local aggressive factors, but the formation of submucous nodes that determines the occurrence of gastric ulcers. Therefore, H. pylori has a dose-effect on only duodenal ulcers, whereas gastric ulcers’ association with H. pylori is less clear. |
Article 2, Page 19, Right Column, Lines 3-12. |
|
|
48. Only 27% of symptomatic children with peptic ulcers were H. pylori positive. |
|
|
|
49. 48% of patients developed ulcers within six months of healing, but the re-infection rate after eradication was very low (<2%). |
|
|
|
50. In developing countries with uniformly high prevalence of H. pylori infection, there are marked regional differences in the prevalence of duodenal ulcers, which could not be explained by the more toxic CagA and VacA H. pylori strains. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
51. In the countries with low prevalence of H. pylori, 30%-40% or more of duodenal ulcer patients are H. pylori-negative, and the absence of H. pylori infection in early cases of duodenal ulcers was also reported. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration. Cases D, F, L, and N support the finding that in some countries, 30%-40% of duodenal ulcer 386 patients were H. pylori-negative and explain a clinical observation that up to 35% of 387 infected patients failed to respond to standard anti-H. pylori therapy. |
Article 1, Page 8, Left Column, Lines 2-16; Article 1, Page 8, Right Column, Lines 19-27. |
|
52. The role of H. pylori in peptic ulcers is controversial. |
Without the CCR, there is no benchmark to identify the cause of disease, and the methodologies essential for data analysis have never been established, resulting in many unsolved mysteries and massive challenges. No longer controversial after the application of the CCR. |
Article 1, Discu, Page 9, Left Column, Lines 43-53; Article 1, Discu, Page 9, Right Column, Lines 19-43. |
|
53. ‘H. pylori is the most important aetiological factor so far described for duodenal ulcer’. |
This is a wrong statement. The hyper-secretion of gastric acid is a determinant factor in the late phase of duodenal ulceration; Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, suggesting it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duodenal ulcers. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
54. How H. pylori infection can lead to ulceration is unknown. |
This statement is based on a wrong assumption. Without the hypersecretion of gastric acid, the corrosive intensity caused by either H. pylori or NSAIDs could not reach the threshold of ulceration. H. pylori alone cannot lead to ulceration and thus, the etiology based on H. pylori infection would never be able to explain peptic ulcerations. |
Article 1, Page 7, Right Column, Lines 44-53. |
|
55. No H. pylori, No Ulcer; peptic ulcer is an infectious disease. |
These are wrong statements. Neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 38-48. |
|
56. In spite of a high prevalence of H. pylori infection worldwide, the incidence of duodenal ulcer disease in both adults and children is low in comparison. |
Case B is applicable to most H. pylori infected individuals, but only those also impacted by the hyper-secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. |
Article 1, Page 8, Left Column, Lines 17-23. |
|
57. Kato and colleagues’ retrospective analysis found that H. pylori prevalence in gastric ulcer did not reach 50%; they concluded while H. pylori infection appears to be a risk factor in gastric ulcer, other causes are responsible for most cases. Only 56-96% of gastric ulcer patients are H. pylori-positive, so other factors must be involved. |
The formation of submucous nodes is irrelevant to H. pylori infection, but determined by only the pathogenic nerve impulses from the CNS. Without infection, gastric ulcers may occur if the individual is severely impacted by psychological stress. Therefore, more than 50% of clinical gastric ulcer patients can be H. pylori- negative. The pre-existed pathological lesions in the gastric wall due to psychological stress account for the other unidentified factors. On the other hand, because gastric ulceration is determined not by H. pylori infection, but by the formation of submucous nodes induced by psychological stress, even though the infection rate in the population is as high as 90%, only the individuals affected by psychological stress become ulcer patients, leading to the low incidence of gastric ulcers despite a high prevalence of H. pylori infection. |
Article 2, Page 19, Left Column, Lines 32-49. |
|
58. Despite the fall in prevalence of H. pylori infection, the attributable risk of H. pylori infection in peptic ulcer disease has not changed. |
Since H. pylori infection is not the cause of peptic ulcers, the attempt to explain an epidemiological observation by H. pylori infection would inevitably result in the inconsistency. |
Article 2, Page 19, Left Column, Line 49-Right Column, Line 2. |
|
59. There was a significantly higher incidence of idiopathic duodenal ulcers in the younger generation. |
The younger the individuals, the less chances they get infected with H. pylori and/or become a NSAIDs users, resulting in the significantly higher incidence of idiopathic [peptic] duodenal ulcers in the younger generation. |
Article 2, Page 19, Right Column, Line 51-Page 20, Left Column, Line 3. |
|
60. There are basically three different types of peptic ulcer: H. pylori-related peptic ulcer; NSAID-related peptic ulcer; and non-H. pylori, non-NSAID ulcer. |
This classification is because the cause of peptic ulcers has never been not identified in modern medicine. This classification overlooks the primary/decisive factor in the occurrence of duodenal ulcers, the hypersecretion of gastric acid. |
Article 1, Page 8, Right Column, Lines 14-18. |
|
61. A relatively isolated group of Australian aboriginals have virtually no H. pylori infection and hardly any peptic ulcer disease. |
|
|
|
62. Up to 20% of patients with ulcers suffer a relapse of ulcer disease despite successful eradication of their infections, suggesting that H. pylori was not the cause of their original ulcers. |
Cases D and F were caused simply by the hypersecretion of gastric acid due to psychological stress, which explain 20%-40% of patients with idiopathic ulcers (H. pylori-negative and non-NSAIDs user) and the eradication of H. pylori can not prevent the relapse of these cases. |
Article 1, Page 8, Left Column, Lines 42-46. |
|
63. Difference in virulence of H. pylori strains (cag- and cag+) has been considered as a putative explanation as to why only a minority of infected population develop peptic ulcers. |
H. pylori infection is not the cause of duodenal ulcers but plays a secondary role in only the late phase of ulceration and thus, H. pylori strains such as CagA, VacA, and SecA, cannot explain the higher prevalence of duodenal ulcers. |
Article 1, Page 8, Left Column, Lines 2-16. |
|
64. H. pylori infection in rats was successful and was accompanied by a mild to moderate mucosal inflammation. After H. pylori inoculation, an ulcer was induced in the oxyntic mucosa of both infected and uninfected rats by exposing the serosal side to acetic acid. |
For those individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating that gastric acid plays a more important role than H. pylori in duodenal ulcerations. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
65. More than 95 percent of patients with duodenal ulcers and more than 80 percent of patients with gastric ulcers are infected with H. pylori. |
|
|
|
66. The corresponding ulcer areas in the H. pylori-infected rats were significantly larger in the infected than in the uninfected rats, and ulcer healing was delayed in the infected rats. Eliminating H. pylori accelerates the healing of ulcer. |
Only after the submucous nodes have come into being, could H. pylori have the chance to corrode the tissues at the site, enlarging the lesions and delaying the regeneration and rehabilitation of local tissues. Eradicating H. pylori attenuates the impact of local aggressive factors, is conducive to the regeneration and rehabilitation of local tissues, and attenuate or inhibit ulcer symptoms, resulting in resolution and less medical visits. |
Article 2, Page 19, Left Column, Lines 18-31; Article 2, Page 18, Left Column, Lines 42-49. |
|
67. Eradication of H. pylori in gastric ulcer patients has also been shown to be associated with a significant reduction in ulcer relapse rate, compared with those who remain infected. |
Medications, such as proton pump inhibitors for gastric acid reduction and antibiotics for H. pylori eradication, may mitigate symptoms, reduce the morbidity rate, and delay relapse to a certain degree, and many cases were diagnosed as healed, but the real cause of gastric ulcers, psychosocial stress, was not removed. As a result, relapse may occur during treatments. |
Article 2, Page 18, Right Column, Lines 3-10. |
|
68. Clinical data reported that the recurrence rate is as high as 74-80% in H. pylori positive group of duodenal ulcer patients who have healed, but the negative group is only 0-28%. The discrimination was remarkable. |
The eradication of H. pylori would effectively cure the patients without recurrence in Cases G and I, which are representative of most clinical patients. However, the eradication of H. pylori would not prevent the recurrence of ulcers in H. pylori-negative Cases D and F, or in the H. pylori-positive Cases J and R, where the damage caused by the bacterium was not a determinant factor in ulceration. It is more common to identify cases similar to Cases G and I in clinical patients, whereas cases like Cases D, F, J and R occur less frequently, which explains the dramatic decrease of ulcer recurrences after H. pylori eradication. |
Article 1, Page 8, Right Column, Lines 40-53. |
|
69. A negative interaction between H. pylori and NSAIDs on duodenal ulcers suggests that H. pylori reduces the development of ulcers in NSAIDs users. |
H. pylori upregulates the expression of COX-2 and subsequently results in the biosynthesis of gastroprotective prostaglandin, which in turn offsets the corrosive intensity of NSAIDs and thus is conducive to the healing of NSAIDs-induced ulcers, causing ‘H. pylori reduces the development of ulcers in NSAIDs users’. |
Article 1, Page 7, Left Column, Lines 46-52. |
|
70. ~20% of peptic ulcers in the Polish population are unrelated to H. pylori and NSAIDs use (idiopathic ulcers). |
For individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
71. The prevalence of H. pylori in patients with bleeding ulcers may be 15~20% lower than in patients with non-bleeding ulcers. |
Bleeding indicates patients are more likely to be seriously impacted by psychological stress with severe hyperplasia and hypertrophy of parietal and gastrin cells as Cases F and H. pylori infection is not essential for ulceration. In contrast, non-bleeding ulcer suggests the patients are more likely to be slightly impacted by stress with mild hyperplasia and hypertrophy, and H. pylori infection is essential to increase the total corrosive intensity for the induction of ulcers as Case G. As a result, clinical bleeding ulcer patients are more likely to be Case F without H. pylori and non-bleeding patients are more likely to be Case G with H. pylori infection. |
Article 1, Page 8, Left Column, Line 47-Right Colum, Line 7. |
|
72. The eradication of H. pylori reduces the rate of re-bleeding in patients with ulcer disease. |
The eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 41-44. |
|
73. How H. pylori infection affects gastric acid secretion is still unclear. |
The hypersecretion of gastric acid is unrelated to any of the local aggressive factors, such as H. pylori infection, NSAIDs and other medications, but potentiated by the hyperplasia and hypertrophy of one or more endocrine organs and triggered by psychological stress due to personality traits or life events. Thus, ‘H. pylori infection affects gastric acid secretion’ is a wrong assumption. |
Article 1, Page 5, Right Column, Lines 20-35. |
|
74. The incidence of peptic ulcers was higher in H. pylori-infected patients than in the H. pylori-negative group. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/ mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
75. Duodenal acid load determines whether H. pylori can cause duodenal ulcer. |
The hypersecretion of gastric acid is the determinant factor in the late phase of duodenal ulceration, governing multiple characteristics of this disease, especially the observations related to H. pylori and NSAIDs. |
Article 1, Page 5, Right Column, Lines 25-35. |
|
76. The increase in H. pylori density is related to the presence of duodenal ulcer disease. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity, and duodenal ulceration is caused by the total corrosive intensity, the higher the density of H. pylori, the higher total corrosive intensity. As a result, the infection of H. pylori exacerbates clinical symptoms and increases the clinical morbidity/ mortality of the disease. |
Article 1, Page 7, Right Column, Lines 34-41. |
|
77. H. pylori-negative duodenal ulcers were associated with a poorer prognosis mainly because of a higher rate of ulcer and symptom relapse. |
To reach the ulceration threshold without the corrosive intensity from H. pylori, the hypersecretion of gastric acid needs to be higher in H. pylori-negative patients. The higher hypersecretion in Cases D and F indicates more severe negative impacts from psychosocial stress than in Cases G and I. Additionally, the damage from H. pylori can be relieved by antibiotics, as in Cases G and I, decreasing the corrosive intensity in these patients, whereas Cases D and F cannot achieve the same therapeutic effect. Therefore, there is a poorer prognosis and a higher relapse rate in H. pylori-negative patients. |
Article 1, Page 8, Left Column, Lines 31-41. |
|
78. When H. pylori persisted, 61% of duodenal ulcers healed and 84% relapsed. When H. pylori was cleared 92% of ulcers healed and only 21% relapsed during the 12 months follow-up period. |
Since each of the 3 local aggressive factors partially contributes to the corrosive intensity and duodenal ulceration is caused by the total corrosive intensity, the higher density of H. pylori, the higher total corrosive intensity. As a result, H. pylori infection exacerbates clinical symptoms and increases the clinical morbidity/mortality of the disease. In contrast, the eradication of H. pylori decreases the total corrosive intensity, causing mitigated symptoms, lowered morbidity and the rates of re-bleeding in ulcer patients. |
Article 1, Page 7, Right Column, Lines 34-44. |
|
79. Jyotheeswaran and colleagues from greater Rochester, New York, reported a 48% prevalence of H. pylori-negative duodenal ulcers in white patients and 15% in non-white patients, with an overall negative prevalence of 39%. Parsonnet’s meta-analysis indicates the overall prevalence of H. pylori-negative duodenal ulcers is 40%. |
For those individuals with severe hyperplasia and hypertrophy of gastrin and parietal cells, the hypersecretion of gastric acid alone is sufficient to induce duodenal ulcerations. In that case, neither H. pylori infection nor NSAIDs usage is essential for ulceration. Therefore, duodenal ulcers may occur in the absence of H. pylori and/or NSAIDs, leading to idiopathic (H. pylori-negative and non-NSAIDs user) ulcer patients. |
Article 1, Page 5, Right Column, Lines 36-52. |
|
80. A review by van der Voort and colleagues suggests that existing data are consistent with a causal role for H. pylori in stress ulcer formation. |
A statement originated from wrong etiology. ‘A causal role for H. pylori in stress ulcer’ indicates that without stress, H. pylori alone can not induce ulcer. Administering cysteamine or propionitrile, which effectively stimulates the hypersecretion of gastric acid in rats, can induce acute and chronic duodenal ulcers in normal rats, whereas the inoculation of H. pylori alone cannot, further indicating it is not H. pylori but gastric acid that plays a primary/decisive role in the pathogenesis of duodenal ulcer. Case B in Figure 2 is applicable to most H. pylori infected individuals, but only those also impacted by the hyper-secretions of gastric acid due to psychological stress (Case G) will have the chance to become ulcer patients. That explained the wrong statement “a causal role for H. pylori in stress ulcer formation”. |
Article 1, Page 5, Right Column, Lines 43-52. Article 1, Page 8, Left Column, Lines 17-25. |
|
81. Barry Marshall drank a concoction made from cultured H. pylori and came down with gastritis that could be cured with antibiotics. |
|
|